
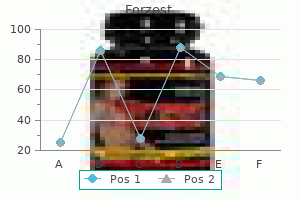
Forzest dosages: 20 mg
Forzest packs: 10 pills, 30 pills, 60 pills
20 mg forzest discount with visa
Efficacy and security of oral naltrexone remedy for pruritus of cholestasis: a crossover erectile dysfunction in diabetes mellitus pdf 20 mg forzest generic with mastercard, double blind impotence questions generic forzest 20 mg fast delivery, placebo-controlled examine. Risk of waitlist mortality in patients with major sclerosing cholangitis and bacterial cholangitis. Endoscopic stent remedy for dominant extrahepatic bile duct strictures in main sclerosing cholangitis. Endoscopic management of biliary tract strictures in primary sclerosing cholangitis. Is there a role for cholangioscopy in sufferers with primary sclerosing cholangitis Prospective analysis of the scientific utility of single-operator peroral cholangioscopy in sufferers with main sclerosing cholangitis. Spanish experience in liver transplantation for hilar and peripheral cholangiocarcinoma. Liver transplantation for main sclerosing cholangitis: predictors and consequences of hepatobiliary malignancy. Recurrence and rejection in liver transplantation for major sclerosing cholangitis. Biliary strictures and recurrence after liver transplantation for major sclerosing cholangitis: a retrospective multicenter evaluation. Clinicopathologic findings of recurrent major sclerosing cholangitis after orthotopic liver transplantation. Risk elements for recurrent major sclerosing cholangitis after liver transplantation. Risk components and prognosis for recurrent primary sclerosing cholangitis after liver transplantation: a nordic multicentre study. Different immunosuppressive regimens and recurrence of main sclerosing cholangitis after liver transplantation. Ulcerative colitis illness exercise as subjectively assessed by patient-completed questionnaires following orthotopic liver transplantation for sclerosing cholangitis. The results of liver transplantation on the medical course of colitis in ulcerative colitis sufferers with primary sclerosing cholangitis. Natural history of established and de novo inflammatory bowel disease after liver transplantation for main sclerosing cholangitis. Progressive primary sclerosing cholangitis requiring liver transplantation is associated with lowered need for colectomy in sufferers with ulcerative colitis. Bile duct accidents during open and laparoscopic cholecystectomy within the laparoscopic era: alarming developments. Does increased experience with laparoscopic cholecystectomy yield more advanced bile duct accidents Microsporidia an infection in sufferers with the human immunodeficiency virus and unexplained cholangitis. Posttransplant biliary complications within the pre- and post-model for end-stage liver disease era. Early hepatic artery thrombosis after liver transplantation: a scientific review of the incidence, end result and danger elements. Portal cavernoma cholangiopathy: consensus statement of a working celebration of the Indian national association for research of the liver. Immunoglobulin G4(+) B-cell receptor clones distinguish immunoglobulin G 4-related disease from major sclerosing cholangitis and biliary/pancreatic malignancies. Increased T-helper 2 cytokines in bile from sufferers with IgG4-related cholangitis disrupt the tight junction-associated biliary epithelial cell barrier. The immunobiology of receptor activator for nuclear issue kappa B ligand and myeloid-derived suppressor cell activation in immunoglobulin G4-related sclerosing cholangitis. Clinical options, response to therapy, and outcomes of IgG4-related sclerosing cholangitis. Utility of serum immunoglobulin G4 in distinguishing immunoglobulin G4-associated cholangitis from cholangiocarcinoma. Analysis of 5 chronic inflammatory illnesses identifies 27 new associations and highlights disease-specific patterns at shared loci. High-dose ursodeoxycholic acid in major sclerosing cholangitis: a 5-year multicenter, randomized, controlled study. Recurrent pyogenic cholangitis with hepatolithiasis-the position of surgical remedy in North America. Perihilar or hilar cholangiocarcinomas come up between secondorder bile ducts and the insertion of the cystic duct. The pure course of cholangiocarcinoma is aggressive, with a median survival of lower than 24 months following analysis. The highest incidence is observed in Southeast Asia, with age-adjusted incidence rates up to 113 per one hundred,000 inhabitants, and the bottom incidence is noticed in Australia, with charges as little as 0. The second version of the International Classification of Disease for Oncology categorised Klatskin tumors as intrahepatic. Biliary malignancies comprise the vast majority of biliary neoplasms and are divided into 3 classes: (1) carcinomas of the intra- and extrahepatic bile ducts (cholangiocarcinomas), (2) carcinoma of the gallbladder, and (3) carcinoma of the ampulla of Vater. Cholangiocarcinomas are additional categorised into intrahepatic, perihilar, and distal cholangiocarcinoma on the premise of their anatomic location inside the biliary treetract. In sure components of the world, nevertheless, their prevalence charges are high, making them main causes of most cancers death in these areas. Each anatomic subtype has a definite epidemiology, pathogenesis, danger components, management, and prognosis. A, Anatomic classification of intrahepatic, perihilar, and distal cholangiocarcinoma. Established Risk Factors Although there are a quantity of known danger elements for cholangiocarcinoma, most instances are sporadic and happen within the absence of a known risk issue. Heavy alcohol consumption has been associated both with intrahepatic and with perihilar and distal cholangiocarcinoma and is believed to be a probable threat issue. Macroscopically, intrahepatic cholangiocarcinomas can have 3 subtypes: mass-forming, periductal-infiltrating, and intraductal development type. The mass-forming sort is the most typical type of intrahepatic cholangiocarcinoma, accounting for more than 85% of instances. Because perihilar cholangiocarcinomas have a tropism for bile, the initial growth pattern is often periductal, and with tumor development, a mass lesion is shaped leading to a mass-forming and periductal-infiltrating lesion. Other histologic types include intestinal-type adenocarcinoma, clear cell adenocarcinoma, signet-ring cell carcinoma, adenosquamous carcinoma, squamous cell carcinoma, and small cell carcinoma. Clinical Features and Diagnosis the prognosis of cholangiocarcinoma is difficult because the presentation is usually insidious, and the outcomes of diagnostic research are incessantly nonspecific.
Cheap 20 mg forzest overnight delivery
World Health Organization classification of tumours: Pathology and genetics of tumours of the digestive system erectile dysfunction treatment in the philippines forzest 20 mg visa. Prognostic factors in resected pancreatic adenocarcinoma: evaluation of precise 5-year survivors impotence ultrasound forzest 20 mg order overnight delivery. The chromatin regulator Brg1 suppresses formation of intraductal papillary mucinous neoplasm and pancreatic ductal adenocarcinoma. Classification, Morphology, molecular pathogenesis, and outcome of premalignant lesions of the pancreas. Improving the diagnostic yield from staging laparoscopy for periampullary malignancies: the value of preoperative inflammatory markers and radiologic tumor size. Prospective evaluation of advanced molecular markers and imaging strategies in patients with indeterminate bile duct strictures. Resected adenocarcinoma of the pancreas-616 patients: results outcomes and prognostic indicators. Vein involvement during pancreaticoduodenectomy: is there a need for redefinition of "borderline resectable illness" Do preoperative biliary stents enhance postpancreaticoduodenectomy issues Effect of biliary decompression on morbidity and mortality of pancreaticoduodenectomy. Does revision of resection margins primarily based on frozen section improve total survival following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma A population-based, case-controlled examine of polymorphisms in carcinogen-metabolizing genes, smoking, and pancreatic adenocarcinoma threat. A prospective randomized trial comparing commonplace pancreatoduodenectomy with pancreatoduodenectomy with prolonged lymphadenectomy in resectable pancreatic head adenocarcinoma. A potential randomized controlled examine comparing outcomes of standard resection and prolonged resection, together with dissection of the nerve plexus and numerous lymph nodes, in sufferers with pancreatic head cancer. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical remedy of adenocarcinoma of the pinnacle of the pancreas: a multicenter, potential, randomized examine. Yield of endoscopic ultrasound-guided nice needle aspiration and endoscopic retrograde cholangiopancreatography for strong pancreatic neoplasms. Pancreatico-biliary endoscopic ultrasound: a systematic evaluation of the levels of proof, performance, and outcomes. Repeat endoscopic ultrasoundguided nice needle aspiration for solid pancreatic neoplasms at a tertiary referral center will alter the initial inconclusive outcome. Unnecessary exams and procedures in sufferers presenting with strong tumors of the pancreas. Pancreaticoduodenectomy with or with out distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Use and outcomes of consensus definitions in pancreatic surgical procedure: a scientific evaluation. Enteral and parenteral nutrition in the conservative therapy of pancreatic fistula: a randomized medical trial. Effect of hospital volume, surgeon experience, and surgeon quantity on affected person outcomes after pancreaticoduodenectomy: a single-institution experience. Minimally invasive versus open pancreaticoduodenectomy: a propensity-matched research from a nationwide cohort of patients. A modern evaluation of survival for resected pancreatic ductal adenocarcinoma. Survival after resection of pancreatic adenocarcinoma: outcomes from a single establishment over three a long time. Pancreatic ductal adenocarcinoma: is there a survival difference for R2 resections versus domestically superior unresectable tumors Fluorouracil vs gemcitabine chemotherapy earlier than and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized managed trial. Surgical administration of patients with unresectable pancreatic adenocarcinoma: Trends and Lessons Learned from a big, single establishment experience. Long-term outcome of biliary and duodenal stents in palliative treatment of patients with unresectable adenocarcinoma of the head of the pancreas. Covered metal versus plastic stents for malignant frequent bile duct stenosis: a prospective, randomized, managed trial. Fully coated self-expandable metallic stents are effective and secure to deal with distal malignant biliary strictures, irrespective of surgical resectability standing. Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer Prospective analysis of laparoscopic celiac plexus block in patients with unresectable pancreatic adenocarcinoma. An open randomized comparability of medical effectiveness of protocol-driven opioid analgesia, celiac plexus block, or thoracoscopic splanchnicectomy for ache management in patients with pancreatic and other stomach malignancies. Treatment of regionally unresectable carcinoma of the pancreas: comparability of combinedmodality therapy (chemotheraphy plus radiotherapy) to chemotheraphy alone. Cystic tumors of the pancreas and tumor-like lesions with cystic options: a evaluation of 418 circumstances and a classification proposal. Mucin-producing neoplasms of the pancreas: an analysis of distinguishing medical and epidemiological characteristics. Mucinous cystic neoplasms of the pancreas with overt and latent malignancy (cystadenocarcinoma and cystadenoma). International consensus pointers for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Laparoscopic vs open distal pancreatectomy: a single-institution comparative examine. Laparoscopic distal pancreatectomy is associated with significantly much less total morbidity in comparability with the open method: a systematic evaluate and meta-analysis. Enucleation in pancreatic surgical procedure: indications, method, and outcome in comparison with commonplace pancreatic resections. Resected serous cystic neoplasms of the pancreas: a evaluate of 158 patients with recommendations for remedy. Improvements in survival and scientific benefit with gemcitabine as first-line therapy for sufferers with superior pancreas most cancers: a randomized trial. Extended neoadjuvant chemotherapy for borderline resectable pancreatic cancer demonstrates promising postoperative outcomes and survival. Preoperative/ neoadjuvant remedy in pancreatic cancer: a scientific evaluate and meta-analysis of response and resection percentages. Serous cystadenoma of the pancreas: Appraisal of active surgical strategy before it causes issues.
Diseases
- Spasticity multiple exostoses
- Encephalocele frontal
- Cutis laxa osteoporosis
- Congenital stenosis of cervical medullary canal
- Hypotrichosis
- Meacham Winn Culler syndrome
- Chronic fatigue syndrome
- Porphyria, hereditary coproporphyria
- Hypertelorism hypospadias syndrome
20 mg forzest mastercard
Recurrent acute pancreatitis: worldwide state-of-the-science conference with suggestions impotence at 30 cheap forzest 20 mg without a prescription. The precision medication initiative cohort program-building a analysis basis for twenty first century medication doctor for erectile dysfunction in chennai forzest 20 mg cheap free shipping. Precision Medicine Initiative Work Group Report to Advisory Committee to the Director: 2015 September 17 2015. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by worldwide consensus. Determinant-based classification of acute pancreatitis severity: a global multidisciplinary session. Ethanol diet will increase the sensitivity of rats to pancreatitis induced by cholecystokinin octapeptide. Intra-acinar trypsinogen activation mediates early phases of pancreatic damage but not inflammation in mice with acute pancreatitis. Mechanisms of disease: advances in understanding the mechanisms leading to chronic pancreatitis. Mitochondrial dysfunction, through impaired autophagy, leads to endoplasmic reticulum stress, deregulated lipid metabolism, and pancreatitis in animal models. A sign peptide cleavage web site mutation in the cationic trypsinogen gene is strongly associated with chronic pancreatitis. Known genetic susceptibility components for chronic pancreatitis in sufferers of European ancestry are uncommon in patients of African ancestry. Chronic alcohol consumption accelerates fibrosis in response to cerulein-induced pancreatitis in rats. Progressive disruption of acinar cell calcium signaling is an early characteristic of ceruleininduced pancreatitis in mice. The function of intracellular calcium signaling in premature protease activation and the onset of pancreatitis. Bile acids induce calcium indicators in mouse pancreatic acinar cells: implications for bile-induced pancreatic pathology. Bile acids induce necrosis in pancreatic stellate cells dependent on calcium entry and sodium-driven bile uptake. Elevated pancreatic secretory trypsin inhibitor levels throughout severe inflammatory disease, renal insufficiency, and after varied surgical procedures. Determinants of chymotrypsin C cleavage specificity within the calcium-binding loop of human cationic trypsinogen. Environmental and genetic stressors and the unfolded protein response in exocrine pancreatic function-a speculation. Autophagy, inflammation, and immune dysfunction within the pathogenesis of pancreatitis. Autophagic cell dying of pancreatic acinar cells in serine protease inhibitor Kazal type 3-deficient mice. Pancreatic lipomatosis is a structural marker in nondiabetic children with mutations in carboxyl-ester lipase. Diagnosis of cystic fibrosis: consensus tips from the cystic fibrosis foundation. Genotypes and phenotypes in cystic fibrosis and cystic fibrosis transmembrane regulator-related disorders. Cystic fibrosis transmembrane conductance regulator-related metabolic syndrome and cystic fibrosis display screen positive, inconclusive diagnosis. Immunohistochemical research of secretory proteins within the growing human exocrine pancreas. Pancreatic features of cystic fibrosis and different inherited causes of pancreatic dysfunction. Identification of common cystic fibrosis mutations in African-Americans with cystic fibrosis increases the detection fee to 75%. Pancreatitis in hispanic sufferers with cystic fibrosis carrying the R334W mutation. Cystic fibrosis: a evaluate of associated phenotypes, use of molecular diagnostic approaches, genetic traits, progress, and dilemmas. Bellanne-Chantelot C, Schmaltz-Panneau B, Marty C, Fenneteau O, Callebaut I, Clauin S, et al. Johanson-Blizzard syndrome: expanding the phenotype of exocrine pancreatic insufficiency. Bicarbonate-rich fluid secretion predicted by a computational mannequin of guinea-pig pancreatic duct epithelium. Ductal mucus obstruction and reduced fluid secretion are early defects in continual pancreatitis. New York, Heidelberg, Dordrecht, London: Springer/American Physiological Society; 2016. Relation between mutations of the cystic fibrosis gene and idiopathic pancreatitis. Molecular and functional identification of a Ca2+ (polyvalent cation)-sensing receptor in rat pancreas. Molecular mechanisms of calcium-sensing receptor-mediated calcium signaling within the modulation of epithelial ion transport and bicarbonate secretion. Disorders of the calciumsensing receptor and companion proteins: insights into the molecular foundation of calcium homeostasis. Targeted gene next-generation sequencing in Chinese youngsters with persistent pancreatitis and acute recurrent pancreatitis. Molecular foundation for cation selectivity in claudin-2-based paracellular pores: identification of an electrostatic interplay website. Claudin-1, claudin-2 and claudin-11 genes differentially affiliate with distinct forms of anti-inflammatory macro- 892. Do pancreatic cancer and continual pancreatitis share the identical genetic risk elements Lipotoxicity causes multisystem organ failure and exacerbates acute pancreatitis in obesity. Evaluation and remedy of hypertriglyceridemia: an Endocrine Society clinical practice guideline. Effect of serum triglycerides on medical outcomes in acute pancreatitis: findings from a regional integrated health care system. Elevated serum triglycerides are independently related to persistent organ failure in acute pancreatitis. Stratified analysis and medical significance of elevated serum triglyceride ranges in early acute pancreatitis: a retrospective research. Mutations in exon three of the lipoprotein lipase gene segregating in a household with hypertriglyceridemia, pancreatitis, and noninsulin-dependent diabetes. Incidence of pancreatitis, secondary causes, and treatment of patients referred to a specialty lipid clinic with extreme hypertriglyceridemia: a retrospective cohort research. Excess of uncommon variants in genes identified by genome-wide association research of hypertriglyceridemia. Evolving roles for physicians and genetic counselors in managing advanced genetic problems.
Forzest 20 mg order with visa
An intensive literature has compared these therapies erectile dysfunction age 32 forzest 20 mg order line, culminating in a multicenter European randomized controlled trial erectile dysfunction weight loss forzest 20 mg purchase overnight delivery, which concluded that each approaches have been about 90% efficient with no statistically important distinction between them. Subsequently, a considerable amount of retrospective data and a reassessment of the European achalasia trial85 suggest that achalasia subtype is of nice relevance in determining remedy effectiveness. The bulk of the literature pertinent to achalasia therapy is composed of uncontrolled case series using a big selection of qualitative endpoints as indications of efficacy. As already noted, there has been minimal standardization as to the factors for outlining achalasia, illness severity, or the technical particulars of how the remedies are performed. Furthermore, some series have been collected prospectively, some retrospectively, and a few a combination. Hypopharyngeal (Zenker) Diverticula and Cricopharyngeal Bar the remedy of hypopharyngeal diverticula is cricopharyngeal myotomy with or and not using a diverticulectomy or diverticulopexy. Good or excellent results are reported in 80% to 100 percent of Zenker sufferers handled by transcervical myotomy mixed with diverticulectomy or diverticulopexy. There are situations during which a limited procedure could be adequate, however a definitive approach to the issue of pulsion diverticula ought to contain both diverticulectomy and myotomy. A newer pattern is to deal with Zenker diverticula through both rigid or flexible endoscopy. With each strategies, the precept is to divide the septum between the lumen of the diverticulum and the lumen of the esophagus. The division allows meals and liquid to flow out of the diverticulum distal to the cricopharyngeus (which was throughout the septum) somewhat than to accumulate throughout the diverticulum. Amyl nitrite, sublingual nitroglycerin, theophylline, and 2-adrenergic agonists have also been tried. The largest reported experience has been with isosorbide dinitrate (Isordil) and nifedipine. However, the unwanted effects of nitrates, notably headache, are common and the efficacy may be very limited. With calcium channel blockers (mainly nifedipine) the limiting unwanted side effects are flushing, dizziness, headache, peripheral edema, and orthostasis. Sublingual nifedipine (30 to 40 mg/day) administered before meals was studied in 29 sufferers with early achalasia and was considerably higher than placebo, with good ends in 70% of achalasics followed for six to 18 months. Although conceptually interesting, the practicality of utilizing sildenafil clinically is limited by its cost and potential unwanted effects. Side results are rare however can include chest discomfort for several days and occasional rash. Only dilators particularly designed to deal with achalasia achieve enough diameter for lasting profit; dilation to a lesser diameter provides solely very short-term benefit at greatest. These are lengthy, noncompliant, cylindrical balloons which have radio-opaque markings. Once positioned, the balloon is inflated to full diameter utilizing a handheld manometer taking care to visualize the indentation of the sphincter on the balloon floor because it expands. Pneumatic dilation is usually done on an outpatient basis with the patient beneath aware sedation. However, the strategy of pneumatic dilation is extremely variable among practitioners in terms of affected person preparation, parameters of balloon inflation, and postdilation monitoring. The main complication of pneumatic dilation is esophageal perforation, with a reported incidence ranging between 0% and 5% and a world average of 1%. Alternatively, some practitioners routinely obtain a fluoroscopic examination of the esophagus following pneumatic dilation to be certain that perforation has not occurred. However, if a perforation is substantial, or if worsening chest ache and fever occur, surgical restore ought to be pursued expediently. The scientific efficacy reported for dilation ranges extensively from 32% to 98%, likely because of the intense variability in technique, methods for assessing remedy end result, and the acceptability of performing repeated dilations over time. Heller Myotomy Current surgical procedures for treating achalasia are variations on the esophagomyotomy described by Heller in 1913. Although clearly efficacious, open Heller myotomy is related to appreciable morbidity associated to the thoracotomy. However, adoption of the laparoscopic method for achalasia surgical procedure has largely mitigated this. Published sequence of the efficacy of Heller myotomy in treating achalasia report good to wonderful ends in 62% to one hundred pc of sufferers, with persistent dysphagia in fewer than 10%. The laparoscopic strategy is associated with comparable efficacy, reduced morbidity, and shorter hospital keep in comparison with myotomy through thoracotomy, laparotomy, or thoracoscopy. Thus, laparoscopic Heller myotomy mixed with a partial fundoplication (Toupet or Dor) has turn out to be the preferred surgical procedure for achalasia. An unsatisfactory end result following Heller myotomy may result from incomplete myotomy, scarring of the myotomy, useful esophageal obstruction from the antireflux element of the operation, paraesophageal hernia, or extreme esophageal dilatation. There was no difference in success rates after 2 years of follow-up: 92% for pneumatic dilation versus 87% for laparoscopic myotomy. Hence, one ought to assess the available local assets, as properly as patient preference, in choosing the preliminary remedy. Treatment Failures Persistent dysphagia after achalasia therapy suggests remedy failure and must be evaluated with some combination of endoscopy, high-resolution impedance manometry,ninety seven useful luminal imaging probe,ninety eight and fluoroscopic imaging. Endoscopy might detect esophagitis, stricture, paraesophageal hernia, or anatomic deformity. Impedance manometry could additionally be useful to quantify persistent or recurrent sphincter dysfunction, distal spasm, or esophageal retention. Reoperation, in general, is much less effective than an preliminary operation for any indication in achalasia. Occasionally, patients fail to reply to optimally carried out dilation or myotomy and require alternative treatment. In extremely advanced or refractory circumstances of achalasia, esophageal resection with gastric pull-up or interposition of a phase of transverse colon or small bowel could be the only possibility. Indications for this intervention embrace unresolvable obstructive symptoms, malnutrition, bleeding, chronic aspiration, cancer, and perforation throughout dilation. Although wonderful long-term functional outcomes could be achieved, the reported mortality of this surgical procedure is about 4%, according to esophagectomy accomplished for other indications. Risk of Squamous Cell Cancer Squamous cell carcinoma might develop in the achalasic esophagus. The tumors develop many years after the analysis of achalasia and often arise in a tremendously dilated esophagus with stasis esophagitis. Symptoms attributable to the most cancers could be delayed, and the neoplasms are often massive and superior at the time of detection raising the difficulty of surveillance endoscopy. However, an analysis of a database encompassing the complete Swedish population of 1062 achalasics means that after discounting incident carcinomas, the overall squamous cell cancer risk for achalasics was 17-fold compared to age-matched controls, leading to a 0. The authors calculated that if surveillance endoscopy was done annually, 406 exams would have to be done in men and 2220 in ladies earlier than 1 potentially treatable tumor was discovered. However, even that calculation is optimistic, given that detection of a small most cancers in a massively dilated esophagus with retained food and stasis esophagitis is way from assured. However, they also state that if surveillance was considered, it will be affordable to begin 15 years after the onset of achalasia symptoms.
Forzest 20 mg without prescription
This typically entails sectioning the higher splanchnic nerve on one or each side jacksonville impotence treatment center forzest 20 mg buy otc. Pain relief after thoracoscopic splanchnicectomy averages about 50% at 1 12 months and drops to 25% with longer follow-up erectile dysfunction use it or lose it order 20 mg forzest. Another method to minimizing nociception focuses on the central nervous system and pain notion. The first step is to ensure the prognosis is right, which may be difficult in less-advanced continual pancreatitis. It is prudent to assess for particularly treatable problems that may trigger pain, similar to gastric, duodenal, or biliary obstruction, pseudocyst, or secondary most cancers. A heart-healthy or Mediterranean food plan is reasonable, with avoidance of meals which cause symptoms. There are several potential explanations for failure of enzyme therapy for steatorrhea. The most typical is inadequate dose, usually due to patient noncompliance with the variety of pills, or the worth of tablets, that must be taken. Changing to a stronger preparation to cut back the variety of pills taken can be useful. It can be necessary to ensure that acid suppression has been prescribed and is being used by patients on the non�enteric-coated preparation. In some sufferers, the enteric-coated preparations might release enzymes within the mid or distal small bowel and this delayed release may not be adequate to effectively treat steatorrhea. In long-standing diabetes, applicable monitoring for nephropathy, retinopathy, and neuropathy is indicated. They happen in about 25% of sufferers with chronic pancreatitis, and are mostly seen in alcoholic chronic pancreatitis. Less common manifestations are a palpable mass, nausea and vomiting (due to compression of the stomach or duodenum), jaundice (due to compression of the bile duct), and bleeding. Elevations in serum lipase and amylase values are found in at least one half of patients, and a persistent elevation in serum lipase or amylase could be a clue to the presence of a pseudocyst. Complications embody compression of large peripancreatic vessels, abdomen, or duodenum; an infection; hemorrhage; and growth of a fistula. Unlike fluid collections and pseudocysts associated with acute pancreatitis, these occurring in a background of chronic pancreatitis resolve far much less commonly. Therapy for symptomatic, sophisticated, or quickly enlarging pseudocysts may be surgical, percutaneous, or endoscopic. Percutaneous tube drainage of pseudocysts is feasible if a protected tract to the collection could be identified. Percutaneous drainage of pancreatic pseudocysts complicating chronic pancreatitis is discouraged owing to the widely held view that such cysts are regularly associated with ductal obstruction downstream from the fluid assortment, making the dangers of fistula formation alongside the tract and of pseudocyst recurrence or continual fistula after removal of the tube unacceptably excessive. The long-term success of percutaneous drainage remains to be unknown but is actually comparatively low. Re-accumulation of the gathering after tube removal Diabetes Mellitus Periodic monitoring for the development of diabetes is acceptable in patients with persistent pancreatitis. Morbidity and mortality due to diabetes mellitus might happen from progressive microangiopathic problems or from more dramatic problems, similar to treatment-induced hypoglycemia (in these with inadequate glucagon reserve and particularly in those who are malnourished). Some sufferers show response to the usage of an oral hypoglycemic, corresponding to a sulfonylurea, thiazolidinedione, metformin, or other agents. Complications, which happen in lower than 10% to 15% of circumstances, embody bleeding, an infection of the cavity, and formation of a draining fistula along the tube tract. Endoscopic remedy of pseudocysts is feasible if the fluid collection may be accessed via the papilla or through the wall of the abdomen or duodenum. Transpapillary drainage is feasible for smaller pseudocysts within the head of the gland that talk with the pancreatic duct. All others that are amenable to endoscopic therapy are higher managed with endoscopic cystogastrostomy or cystojejunostomy, relying on their location. Antibiotic coverage and available surgical backup are important if endoscopic therapy is undertaken. Typically, stents are left in place for several weeks, or longer, to permit the pseudocyst to decompress. Surgical remedy usually entails cyst decompression right into a loop of small bowel or abdomen, often coupled with a pancreatic ductal drainage procedure. Surgical remedy has a long-term success fee of round 90% and an operative mortality of lower than 3%. This is true of all therapies for pseudocysts, in that pain from the underlying chronic pancreatitis may also happen in the absence of a pseudocyst. Surgical remedy can additionally be necessary in patients who experience extreme complications of less-invasive endoscopic or percutaneous treatments. Cystogastrostomy and cystojejunostomy can be carried out with laparoscopic methods. Endoscopic therapy is vulnerable to a similar downside except these anatomic issues are dealt with. This might cut back the danger of pseudocyst recurrence after elimination of the transenteric pseudocyst stents. Pseudocysts account for 90% of all cystic collections associated with the pancreas. Others occur as a direct result of the pancreatitis, most notably bleeding from a pancreatic pseudocyst, pseudoaneurysm, and portal or splenic vein thrombosis. Bleeding happens from small vessels (venous, capillary, or arteriole) in the wall, which may lead to enlargement of the pseudocyst and further rupture of these small vessels. Pseudoaneurysm Pseudoaneurysms kind as a consequence of enzymatic and stress digestion of the muscular wall of an artery by a pseudocyst. The pseudoaneurysm might rupture both into the pseudocyst (converting the pseudocyst into a bigger pseudoaneurysm) or directly into an adjacent viscus, peritoneal cavity, or pancreatic duct. Pseudoaneurysmal bleeding could complicate 5% to 10% of all circumstances of chronic pancreatitis with pseudocysts, although pseudoaneurysms may be seen in up to 21% of sufferers with persistent pancreatitis present process angiography. Many visceral arteries may be concerned, the splenic artery being commonest, followed by gastroduodenal or pancreaticoduodenal arteries. Although death from a pseudocyst is rare, greater than half the general mortality of pseudocysts is as a outcome of of hemorrhage. In many cases, an initial self-limited bleed occurs (so-called sentinel bleed), adopted hours or days later by a large exsanguinating hemorrhage. The initial self-limited nature of the bleed may be due to transient tamponade of the bleeding inside the confines of the pseudocyst. If no obvious bleeding web site is seen, pseudoaneurysm formation ought to be thought-about. Once a pseudoaneurysm has been identified, it ought to be handled whether or not or not it has triggered bleeding. Angiographic embolization or stentgraft placement has largely changed major surgery371,372 which is reserved for instances in which these therapies have failed. Variceal Bleeding From Splenic Vein Thrombosis Variceal bleeding may complicate continual pancreatitis because of either associated alcoholic cirrhosis or thrombosis of the splenic (and, much less generally, portal) vein.
Syndromes
- Generalized malaise
- The pregnancy resulted after a traumatic event such as rape or incest
- Anxiety
- Erythema nodosum
- New blisters or ulcers
- Damage to the womb or cervix
- How long do your periods usually last?
- Do not stop or change your medications without talking to your doctor first.
- Blisters in or around the mouth and throat, causing feeding problems or swallowing difficulty
20 mg forzest otc
A erectile dysfunction pills in pakistan buy discount forzest 20 mg online, Tachygastria erectile dysfunction of diabetes forzest 20 mg cheap with amex, an abnormally rapid signal at 6 cycles per minute (cpm), shown by dots. After ingestion of most stable or liquid meals, a socalled frequency dip happens in the first 10 to quarter-hour after the meal. The frequency dip displays modifications ensuing from marked gastric leisure and lodging of the check meal associated to the quantity or the temperature of the meal. Recordings which have mixtures of tachygastria and bradygastrias are termed nonspecific or mixed gastric dysrhythmias. Slow frequencies are additionally present from 1 to 2 cpm (bradygastrias) and from 4 to 9 cpm (tachygastrias) in sufferers with nausea with or without gastroparesis. The barostat balloon was designed to measure changes in tone (or gastric relaxation) and volume within the more spherical areas of the proximal abdomen. As the fundus and proximal abdomen relax in response to the check meal, more air is concomitantly infused into the balloon to preserve the established baseline intraballoon pressure. Failure of fundic relaxation has also been recorded in patients with gastroparesis. Histopathologic Studies in Gastric and Pyloric Neuromuscular Disorders Efforts to define the histopathologic basis of gastric neuromuscular issues have offered basic data for the evolving area of neurogastroenterology. Thus, these problems could also be considered Cajalopathies or gastric enteric neuropathies or, more probably typically, combinations of both. Results from histochemical studies of full-thickness gastric and pyloric tissue additionally present new instructions for understanding the neuromuscular dysfunction of the abdomen and stimulate ideas for novel therapeutic approaches. In the water-load satiety check, water is consumed over a 5-minute period until the subject feels full. The pylorus is tough to study with reference to fasting and postprandial function in awake topics. At the severe end of the spectrum, antral hypomotility and profound gastroparesis are related to extended postprandial fullness, vomiting, bloating, weight reduction, and malnutrition that will require enteral or parenteral nutritional help. Gastric neuromuscular problems range from irregular fundic leisure and emptying to gastric dysrhythmias and antral hypomotility and gastroparesis. Pyloric sphincter dysfunction, duodenal dysfunction, antroduodenal dyscoordination, and vagal hypersensitivity might all be current in some sufferers with gastric neuromuscular disorders. The pyloric sphincter is a key pathophysiologic think about over 20% of sufferers with gastroparesis. Gastroparesis Gastroparesis means "paralysis" of the abdomen, as outlined by the delayed price of emptying of a normal check meal from the abdomen within the absence of mechanical obstruction. Data from Olmstead County, Minnesota, point out an age-adjusted prevalence of particular gastroparesis of 9. The particular gastroparesis group was established on the basis of ordinary gastric scintigraphy results. These sufferers often have diabetes for greater than 10 years, erratic and elevated glucose ranges, peripheral neuropathy, nephropathy, and heart problems. One necessary manifestation of gastric emptying dysfunction in sufferers with insulin-dependent diabetes is erratic glucose control, particularly with sudden hypoglycemic episodes within the postprandial interval if the usual insulin doses are administered earlier than meals. When postprandial insulin ranges improve following insulin injection and but gastric emptying is delayed, nutrient delivery into the duodenum and intestinal glucose absorption are delayed. Thus, plasma glucose ranges lower in response to the insulin remedy and symptomatic hypoglycemia develops unexpectedly. Hypomotility of the fundus and hypercontractility of the pylorus have been present in db/db mice. Postsurgical Gastroparesis Gastroparesis occurs in a subset of sufferers present process subtle or radical stomach operations that range from vagotomy to fundoplication to antrectomy. Truncal vagotomy produces complicated results on the neuromuscular perform of the abdomen. After vagotomy, the fundus fails to chill out usually after meals, resulting in fast filling of the antrum. But in patients present process intensive resection of the antrum and corpus, prolonged signs and persistent gastric neuromuscular dysfunction are likely. Lower esophageal resection for esophageal most cancers consists of resection of the fundus. Pyloroplasty is performed to facilitate gastric emptying, however the lack of the fundus and variable amounts of the corpus (that might embody the pacemaker region) usually leads to persistent nausea, gastric dysrhythmias, and gastroparesis. Ingested food is retained in the remnant fundus and fails to empty into the corpus203; the corpus fails to mix and empty gastric contents even though the anastomosis is extensively patent. The Roux-en-Y gastroenterostomy operation might result within the Roux syndrome by which postprandial pain, bloating, and nausea develop. Delayed gastric emptying is due to "functional obstruction" by the Roux limb as the neuromuscular dyssynchrony within the Roux limb prevents emptying of the abdomen. In the gastric "sleeve" resection for obesity, two thirds of the abdomen is removed including parts of the fundus, corpus, and antrum. After the sleeve resection, gastric emptying of liquid and stable check meals is accelerated, however there are few research out there for evaluation. Postfundoplication gastroparesis and early satiety, bloating, extended fullness, and nausea could occur. These patients have altered fundic rest, delayed gastric emptying, and gastric dysrhythmias, probably on the premise of vagal nerve damage during or after the fundoplication procedure. Gastric easy muscle dysfunction is another mechanism of delayed gastric emptying in some patients with diabetes. Gastric smooth muscle contractility in diabetic rats is decreased in response to electrical stimulation. Type 2 diabetes mellitus patients with gastroparesis are older, have milder delays in gastric emptying, and extra severe early satiety. This affected person had electrical and contractile abnormalities of the stomach as documented by the tachygastria and gastroparesis. Ischemic gastroparesis is distinct from acute mesenteric ischemia, which presents as an belly catastrophe with an acute stomach and gangrenous small intestine (see Chapter 118). Chronic mesenteric ischemia is often due to progressive atherosclerosis or hyperplasia of the intima of the arteries of the celiac, superior mesenteric, or inferior mesenteric artery. Collaterals of those obstructed arteries kind over time so that neuromuscular function of the stomach is preserved, no less than for some time. Bypass graft surgery or dilatation of the stenotic arteries ends in resolution of signs, eradication of gastric dysrhythmias, and reversal of gastroparesis. Patients with idiopathic (discussed below), diabetic, or postsurgical gastroparesis might have a subtype of gastroparesis-obstructive gastroparesis as a end result of pyloric dysfunction. This subtype is essential because endoscopic and surgical therapies are directed in course of the pylorus. Fixed Pyloric Obstruction Fixed obstructive gastroparesis refers to delayed emptying as a end result of mechanical obstruction at the pylorus or duodenal bulbar or postbulbar space by tumor, persistent peptic ulcer or inflammation, rings, or webs. Gastroparesis may very well be obstructive gastroparesis as a end result of pyloric stenosis or postduodenal bulb cancer.
Forzest 20 mg order fast delivery
Small volumes of gastric contents are sampled from one lumen erectile dysfunction doctor toronto buy forzest 20 mg on-line, the pH is measured erectile dysfunction operation forzest 20 mg on-line, and the contents are returned to the stomach. The second lumen is used to infuse sodium bicarbonate to maintain gastric pH on the meal pH. The amount of bicarbonate required to maintain the pH of gastric contents fixed is a measure of the postprandial acid secretory response. Eradication of Hp both restores somatostatin secretion and lowers basal and stimulated gastrin and acid secretion over time to regular levels in most people, thus providing a everlasting remedy for duodenal ulcer disease. This means that altered gastric mucosal protection may be of major pathophysiologic importance (see Chapter 53). Gastric ulcers have been classified based on their location and concomitant affiliation with duodenal ulcer. These findings may replicate a greater degree and extra generalized mucosal irritation of the oxyntic mucosa with reduced functional parietal cell mass. A number of uncommon circumstances are marked by gastric acid hypersecretion and subsequent peptic ulceration (see Chapter 53). In sufferers with systemic mastocytosis, excessive histamine levels, as a result of elevated numbers of mast cells, repeatedly stimulate parietal cells to secrete acid. It is expressed as the sum of the measured acid output, expressed as mmol H+ per hour, for four consecutive 15-minute durations. Pentagastrin is a manufactured analog of gastrin that incorporates the biologically lively C-terminus sequence. Possible side effects embrace flushing, nausea, abdominal ache, dizziness, and palpitations. Sham Feeding�Stimulated Acid Output the cephalic section of acid secretion whereby the thought, sight, smell, and taste of appetizing food, transmitted through the vagus nerve to gastric enteric neurons, stimulates acid secretion can be studied by sham feeding. Pepsinogens are converted within the gastric lumen by gastric acid to pepsins, which contain 2 active-site aspartate residues. Once this response begins, pepsins can autocatalyze the conversion of pepsinogens to pepsins. Gastric acid not only offers an optimum pH for peptic activity however itself denatures dietary protein, making it more prone to peptic hydrolysis. As mentioned, partially digested protein stimulates gastrin and thus acid secretion. The basis of the secretin test to diagnose gastrinoma is that normally somatostatin cells in the antrum tonically restrain gastrin secretion from G cells. Some information help the uptake of pepsin by epithelial cells in the aerodigestive tract, with possible involvement in carcinogenesis. The properties of gastric lipase are quite distinct from those of pancreatic lipase. Furthermore, safety from peptic proteolysis by an N-glycosylated asparagine at residue 308 permits gastric lipase to retain its exercise in acidic gastric juice (pH 2) despite excessive gastric juice peptic exercise. Aging has been reported to decrease gastric lipase secretion, although data are controversial. Nevertheless, the particular exercise of gastric lipase is equal to or higher than that of pancreatic lipase. Quantitative examine of digestive enzyme secretion and gastrointestinal lipolysis in chronic pancreatitis. The cobalamin-transcobalamin complex is released into the circulation and enters cells by receptor-mediated endocytosis. Once inside cells, cobalamin is dissociated from its transport protein and transformed to its energetic varieties, methylcobalamin and 5-deoxyadenosyl cobalamin. The lively types function coenzymes for methionine synthase and methylmalonyl�coenzyme A mutase, enzymes involved in methylation of homocysteine to methionine and the catabolism of branched-chain amino acids and odd-chain fatty acids in mitochondria, respectively. In the left panel, alkaline mucus secretion and the rate of sloughing into the lumen are balanced. Luminal acid creates a sudden exocytotic burst of mucus secretion from goblet cells and Brunner glands, which thickens the gel (2nd panel). The newly secreted mucus sloughs into the lumen at the next price, leading to a model new steady-state gel thickness (3rd and 4th panels). The authors attributed the observed alterations to upregulation of the kynurenine pathway, speculating that metabolic alterations of this nature may form the idea for biomarker identification. American Journal of Gastroenterology lecture: gastric acid secretion: still relevant Correlative research of hydrochloric acid, pepsin, and intrinsic issue secretion in newborns and infants. Influence of aging, gastric mucosal atrophy, and dietary habits on gastric secretion. Proton pump inhibitors suppress absorption of dietary non-haem iron in hereditary haemochromatosis. Effect of omeprazole on oral iron alternative in patients with iron deficiency anemia. Effects of proton pump inhibitors on calcium carbonate absorption in ladies: a randomized crossover trial. Long-term use of proton pump inhibitors and vitamin B12 status in aged people. Systemic evaluation of the danger of enteric an infection in patients taking acid suppression. L-thyroxine requirement in patients with autoimmune hypothyroidism and parietal cell antibodies. Bacterial killing in gastric juice-effect of pH and pepsin on Escherichia coli and Helicobacter pylori. Clostridium difficile-associated diarrhea and proton pump inhibitor remedy: a meta-analysis. Risk of Clostridium difficile infection with acid suppressing medication and antibiotics: metaanalysis. Proton pump inhibitors and threat of fracture: a scientific evaluation and meta-analysis of observational research. Association of proton pump inhibitor therapy with spontaneous bacterial peritonitis in cirrhotic patients with ascites. Proton pump inhibitors are associated with a excessive rate of great infections in veterans with decompensated cirrhosis. Loss of parietal cell expression of Sonic hedgehog induces hypergastrinemia and hyperprolif- 28. Hepcidin is localised in gastric parietal cells, regulates acid secretion and is induced by Helicobacter pylori infection.

Forzest 20 mg mastercard
In this disease xalatan erectile dysfunction 20 mg forzest order amex, inadequate hepatic copper excretion results in erectile dysfunction 35 year old male buy discount forzest 20 mg online copper accumulation in the liver, brain, kidney, and cornea. Copper in hepatocytes and different cells is sure to metallochaperones, lowmolecular-weight proteins that specifically deliver copper to a goal molecule. In the liver, copper is included into apoceruloplasmin to produce ceruloplasmin (also called holo-ceruloplasmin). More than 90% of the copper in plasma is an integral a half of ceruloplasmin, an 2-glycoprotein that accommodates 6 molecules of copper and has a molecular weight of 132 kd. The regular serum concentration of ceruloplasmin in adults, as measured by immunochemical or enzymatic techniques, is 200 to four hundred mg/L, rising from a very low stage at birth to 300 to 500 mg/L within the first years of life after which settling to adult ranges. Most ingested copper is excreted through the bile; a really small fraction is excreted in urine. When intestinal or liver cells are overloaded with copper, metallothioneins, a class of low molecular-weight cysteine-rich proteins, are induced and sequester copper in a nontoxic type. All functionally essential regions of the gene are conserved between micro organism and yeast. Loosely sure to albumin, and also to histidine and 2macroglobulin, copper is distributed to a wide range of tissues. It is localized in the trans-Golgi community and traffics to cytoplasmic vesicles in the presence of elevated copper. Loosely sure to intracellular metallochaperones (also called copper chaperones), copper is transported to specific proteins, similar to superoxide dismutase in the cytoplasm and various copper-containing proteins in mitochondria. However, with high-throughput testing, the interactome has proved to be extra in depth. A coppertranslocation pathway is shown as eight purple cylinders that span the membrane. Affected dogs show scientific variability that ranges from dying or hepatic illness at 2 to three years of age to much less extreme persistent disease to a high hepatic copper stage. The proposed defective canine gene was recognized by positional cloning; the gene has a deletion of one exon in some,17 but not all, affected dogs. As parenchymal damage progresses, presumably by way of repeated episodes of lobular necrosis, periportal fibrosis develops. Early in the course of Wilson illness, hepatocellular copper is sure mainly to metallothionein and is distributed diffusely in the cytoplasm of hepatocytes; therefore, histochemical stains for copper are negative. As the illness progresses, the copper content material exceeds the storage capability of metallothionein, and copper is deposited in lysosomes. Lysosomal aggregates of copper could be detected by particular staining strategies for copper or copper-binding protein. If the scientific presentation mimics autoimmune hepatitis (see later), a liver biopsy specimen might reveal basic histologic options such as interface hepatitis. Changes in hepatocellular mitochondria, recognized with electron microscopy, are an necessary feature in Wilson illness. The most striking change is dilatation of the tips of the mitochondrial cristae because of separation of the internal and outer membranes of the cristae, with widening of the intercristal area until the looks is irregularly cystic. This finding, although not totally specific for Wilson illness, may be helpful diagnostically, even in younger and minimally affected sufferers. Involvement of hepatocytes may be not uniform, and abnormalities may be present in some hepatocytes in some lobules and not in others. The mitochondrial adjustments are most likely a consequence of oxidative harm from extreme copper in hepatocytes. Hepatic Wilson illness has been identified in toddlers and in sufferers older than age 60. The medical presentation may be as chronic or acute (sometimes rapidly progressive) liver illness, a progressive neurologic dysfunction with out clinically distinguished hepatic dysfunction, isolated acute hemolysis, or psychiatric illness. Wilson disease ought to be thought-about as a possible prognosis in any child, symptomatic or not, with hepatomegaly, persistently elevated serum aminotransferase levels, or evidence of fatty liver. Symptoms may be vague and nonspecific, such as fatigue, anorexia, or stomach ache. Occasional sufferers current with a self-limited clinical sickness that resembles acute hepatitis, with malaise, anorexia, nausea, jaundice, elevated serum aminotransferase ranges, and abnormal coagulation check outcomes. Some sufferers have a historical past of episodic self-limited jaundice, doubtless attributable to hemolysis because of direct toxicity of copper to the erythrocyte membrane. Patients might present with decompensated continual liver disease with hepatosplenomegaly, ascites, a low serum albumin level, and persistently abnormal coagulation check results. Many of these findings relate to portal hypertension as a consequence of Wilson illness quite than to the metabolic dysfunction itself. Wilson disease could current in kids and young adults with clinical liver disease indistinguishable from autoimmune hepatitis (see Chapter 90). Wilson illness have to be specifically ruled out as a result of the therapy of the two illnesses is completely totally different. With applicable therapy, the long-term outlook for patients with Wilson illness that manifests as autoimmune hepatitis appears to be favorable, even if cirrhosis is current. In this "classic Wilsonian acute liver failure," acute Coombs-negative intravascular hemolysis is present, and renal failure may develop. Children with unexplained cholelithiasis, significantly bilirubinate stones, must be examined for Wilson disease. Mood disturbance (mainly melancholy, but typically impulsive or neurotic behavior), deterioration in school efficiency or handwriting, and clumsiness may be identified by cautious direct questioning. A gentle whispery voice (hypophonia) is one other early feature of neurologic involvement. Most sufferers with a neurologic presentation have hepatic involvement, albeit usually asymptomatic. Neurologic involvement follows 1 of 2 primary patterns: a motion disorder or rigid dystonia. A motion disorder tends to occur earlier and consists of tremors, poor coordination, and lack of fine motor management. Spastic dystonic disorders usually develop later, with mask-like facies, rigidity, gait disturbance, and pseudobulbar involvement such as dysarthria, drooling, and swallowing problem. Imaging of the brain is necessary for assessing neurologic Wilson disease, and outcomes could additionally be irregular in the absence of overt neurologic symptoms. Phobias and compulsive behaviors have been reported; aggressive or delinquent habits may also be found. Copper is actually distributed all through the cornea, however fluid streaming favors accumulation close to the limbus, particularly at the superior and inferior poles, and finally circumferentially across the iris. Kayser-Fleischer rings may be absent in 40% to 60% of sufferers with exclusively hepatic involvement and in asymptomatic sufferers. In uncommon individuals with Kayser-Fleischer rings found by the way, Wilson illness must be excluded.
20 mg forzest purchase visa
Pain within the decrease stomach might arise from the rapid spread of pancreatic exudation to the left colon erectile dysfunction and icd 9 generic 20 mg forzest otc. Occasionally www.erectile dysfunction treatment forzest 20 mg free shipping, pain gradually will increase and takes a quantity of hours to reach most intensity. Pain that lasts only a few hours after which disappears suggests a illness other than pancreatitis, such as biliary ache or peptic ulcer. Pain is absent in 5% to 10% of attacks, and a painless presentation could also be a feature of serious deadly disease. Vomiting may be severe, could last for hours, may be accompanied by retching, and may not alleviate pain. Vomiting may be related to severe ache or to inflammation involving the posterior gastric wall. In severe pancreatitis, sufferers look severely unwell and infrequently have abdominal distention, particularly epigastric, which is due to gastric, small bowel, or colonic ileus. Almost all sufferers are tender in the upper abdomen, which may be elicited by gently shaking the abdomen or by mild percussion. Tenderness and guarding can be less than expected, considering the depth of discomfort. Abdominal rigidity, as happens in diffuse peritonitis, is uncommon but may be present, and differentiation from a perforated viscus could also be impossible in these instances. These signs occur in less than 1% of cases and are related to a poor prognosis. A palpable epigastric mass may seem in the course of the disease from a pseudocyst or a large inflammatory mass. The general bodily examination, notably in severe pancreatitis, could uncover markedly abnormal important signs if there are third-space fluid losses and systemic toxicity. Blood strain may be initially greater than normal (perhaps as a end result of pain) after which decrease than regular with third-space losses and hypovolemia. Initially the temperature may be regular, but inside 1 to 3 days it may increase to 101�F to 103�F, owing to the severe retroperitoneal inflammatory process and the discharge of inflammatory mediators from the pancreas. There could also be disorientation, hallucinations, agitation, or coma,178 which can be as a end result of alcohol withdrawal, hypotension, electrolyte imbalance such as hyponatremia, hypoxemia, fever, or toxic results of pancreatic enzymes on the central nervous system. Conjunctival icterus, if present, may be because of choledocholithiasis (gallstone pancreatitis) or bile duct obstruction from edema of the top of the pancreas, or from coexistent liver illness. They often precede abdominal pain or occur without belly ache, however often they seem during a medical episode and disappear with medical improvement. Hepatomegaly, spider angiomas, and thickening of palmar sheaths favor alcoholic pancreatitis. Band keratopathy (an infiltration on the lateral margin of the cornea) happens with hypercalcemia. Microembolization in the retina can lead to typical fundus findings associated with visible disturbances together with blindness. Ecchymosis in the left flank of a 57-year-old man with a 1-week historical past of epigastric ache secondary to acute biliary necrotizing pancreatitis. B, Cullen signal: Ecchymosis and subcutaneous edema within the periumbilical area of a 40-year-old man with alcoholic pancreatitis. It is regularly extreme and epigastric, nevertheless it typically lasts for a number of hours quite than a number of days (see Chapter 65). The pain of a perforated peptic ulcer is sudden, turns into diffuse, and precipitates a inflexible abdomen; movement aggravates pain. Nausea and vomiting happen however disappear soon after onset of pain (see Chapter 53). In mesenteric ischemia or infarction, the clinical setting typically is an older person with atrial fibrillation or atherosclerotic illness who develops sudden ache out of proportion to physical findings, bloody diarrhea, nausea, and vomiting. Abdominal tenderness could also be mild to average, and muscular rigidity will not be extreme regardless of extreme pain (see Chapter 118). In intestinal obstruction, pain is cyclical, belly distention is outstanding, vomiting persists and will turn into feculent, and peristalsis is hyperactive and often audible (see Chapter 123). Because pancreatic diseases enhance serum pancreatic (P) isoamylase, measurement of P-isoamylase can improve diagnostic accuracy. It rises inside 6 to 12 hours of onset and is cleared pretty rapidly from the blood (half-life, 10 hours). The serum amylase is normally elevated on the first day of signs, and it remains elevated for three to 5 days in uncomplicated attacks. Hyperamylasemia can be not specific for pancreatitis; it occurs in lots of conditions. In reality, one half of all sufferers with an elevated serum amylase level might not have pancreatic disease. This has been reported to be as a end result of macroamylasemia (discussed later) or pancreatic hyperamylasemia on a familial foundation. Furthermore, mass lesions such as papillary cystadenocarcinoma of the ovary, benign ovarian cyst, and carcinoma of the lung may cause hyperamylasemia as a end result of they produce and secrete salivary (S-type) isoamylase. Renal failure can improve serum amylase as a lot as 4 to 5 instances the upper restrict of normal due to decreased renal clearance of this enzyme. Chronic elevations of serum amylase (without amylasuria) happen in macroamylasemia. Deliberate contamination of urine with saliva, as in Munchausen syndrome, can increase the urine amylase, with the serum amylase being regular. In the emergency room, pc order set de-selection of amylase however using lipase was an efficient device to scale back non-valueadded testing and scale back price while sustaining quality affected person care and physician alternative in sufferers presenting with stomach ache. Serum lipase is regular when serum amylase is elevated in nonpancreatic situations corresponding to salivary gland disease, amylase-producing tumors, gynecologic conditions similar to salpingitis, and macroamylasemia. Serum lipase all the time is elevated on the primary day of illness and remains elevated longer than does the serum amylase, providing a slightly larger sensitivity. Specificity of lipase can suffer from a few of the same problems as these of amylase, however. In the absence of pancreatitis, serum lipase might improve less than 2-fold above normal in renal insufficiency. Rarely, a nonpancreatic abdominal situation corresponding to small bowel obstruction can increase the serum lipase (and amylase) above 3 times normal. However, when evaluating serum amylase, solely 5% of type 2 diabetics were found to have an elevated stage and no patient had more than 3-fold elevation. It can additionally be potential to analyze serum lipase subtypes such because the pancreatic fraction of the lipase. In addition, an stomach plain film helps exclude different causes of belly ache, corresponding to bowel obstruction and perforation. Gastric abnormalities are brought on by exudate in the lesser sac producing anterior displacement of the abdomen, with separation of the contour of the abdomen from the transverse colon.
Forzest 20 mg buy cheap
Early prediction of long-term survival and the timing of liver transplantation after the Kasai operation erectile dysfunction doctors albany ny forzest 20 mg purchase online. A multicenter examine of the outcome of biliary atresia in the United States erectile dysfunction treatment delhi 20 mg forzest buy amex, 1997 to 2000. Anatomy of the porta hepatis as a foundation for extended hepatoporto-enterostomy for extrahepatic biliary atresia-a new surgical method. Bacterial cholangitis in sufferers with biliary atresia: impact on short-term end result. Prophylactic oral antibiotics in prevention of recurrent cholangitis after the Kasai portoenterostomy. Survival after first esophageal variceal hemorrhage in sufferers with biliary atresia. Portoenterostomy for biliary atresia: long-term survival and prognosis after esophageal variceal bleeding. Sequential remedy of biliary atresia with Kasai portoenterostomy and liver transplantation: a review. The impression of a earlier Kasai procedure on liver transplantation for biliary atresia. One hundred nine living donor liver transplants in adults and children: a single-center expertise. Pediatric liver transplantation for biliary atresia: outcomes of main grafts in 328 recipients. Serial circulating markers of irritation in biliary atresia-evolution of the postoperative inflammatory course of. Extrahepatic anomalies in infants with biliary atresia: results of a big potential North American multicenter examine. Coordinate expression of regulatory genes differentiates embryonic and perinatal forms of biliary atresia. The prognostic worth of ductal plate malformation and other histologic parameters in biliary atresia: an immunohistochemical study. Screening and outcomes in biliary atresia: summary of a National Institutes of Health workshop. Treatment of biliary atresia with particular reference to hepatic porto-enterostomy and its modifications. Prolonged neonatal jaundice and the diagnosis of biliary atresia: a single-center analysis of developments in age at diagnosis and outcomes. Postoperative corticosteroid remedy for bile drainage in biliary atresia-a nationwide survey. Surgical outcome in biliary atresia: etiology affects the affect of age at surgical procedure. Spontaneous perforation of the bile duct in infancy and childhood: a scientific evaluation. Congenital bile duct cysts: classification, operative procedures, and evaluate of thirty-seven cases including most cancers arising from choledochal cyst. Genetic research of congenital bile-duct dilatation identifies de novo and inherited variants in functionally related genes. Predominant extrahepatic biliary disease in autosomal recessive polycystic kidney illness: a new affiliation. Choledochal cyst disease in kids and adults: a 30-year single-institution expertise. Fatty acid calcium stones in sufferers with pancreaticobiliary maljunction/choledochal cyst as another reason for obstructive signs apart from protein plugs. Magnetic resonance cholangiopancreatography of biliary system abnormalities in kids. Characteristics of congenital hepatic fibrosis in a large cohort of patients with autosomal recessive polycystic kidney illness. Autosomal recessive polycystic kidney disease and congenital hepatic fibrosis: abstract assertion of a primary National Institutes of Health/Office of Rare Diseases conference. Autosomal recessive polycystic kidney disease: the scientific experience in North America. Nonsyndromatic paucity of interlobular bile ducts: light and electron microscopic evaluation of sequential liver biopsies in early childhood. Bile duct anomalies in a male youngster with Noonan syndrome: a case for ras and notch pathway synergism. Syndromic paucity of interlobular bile ducts (Alagille syndrome or arteriohepatic dysplasia): evaluation of 80 instances. Alagille syndrome and the notch signaling pathway: new insights into human growth. Proliferation to paucity: evolution of bile duct abnormalities in a case of Alagille syndrome. Embryonic lethality and vascular defects in mice lacking the Notch ligand Jagged1. Peripheral bile duct paucity and cholestasis within the liver of a patient with Alagille syndrome: further evidence supporting a scarcity of postnatal bile duct branching and elongation. Magnetic resonance cholangiopancreatography in primary sclerosing cholangitis in children. The burden of huge and small duct main sclerosing cholangitis in adults and children: a population-based analysis. Primary sclerosing cholangitis in 32 children: scientific, laboratory, and radiographic options, with survival evaluation. Immunomodulatory impact of vancomycin on Treg in pediatric inflammatory bowel disease and first sclerosing cholangitis. Impairment of bone mass improvement in children with chronic cholestatic liver disease. Prevalence of vitamin K deficiency in kids with mild to reasonable chronic liver illness. Novel surgical and pharmacological approaches to continual cholestasis in children: partial external biliary diversion for intractable pruritus and xanthomas in Alagille syndrome. Complementary stimulation of hepatobiliary transport and detoxification techniques by rifampicin and ursodeoxycholic acid in people. The efficacy and security of bile acid binding brokers, opioid antagonists, or rifampin within the treatment of cholestasis-associated pruritus. Colesevelam hydrochloride in scientific apply: a brand new strategy within the therapy of hypercholesterolaemia. Clinical characteristics and risk elements for symptomatic pediatric gallbladder illness. Gallstone prevalence and gallbladder volume in youngsters and adolescents: an epidemiological ultrasonographic survey and relationship to body mass index.