
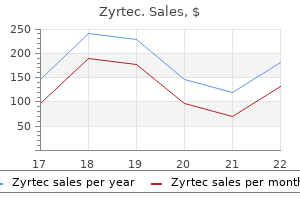
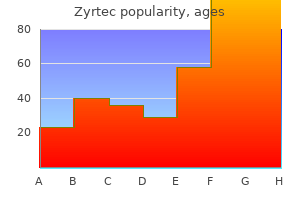
Zyrtec dosages: 10 mg, 5 mg
Zyrtec packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy zyrtec 5 mg low price
The suboccipital surface contains the posterior cerebellar incisura and the vermohemispheric or paravermian fissure, which separates the inferior vermis from the cerebellar hemisphere allergy symptoms spring best 10 mg zyrtec. The components of the inferior vermis and its hemispheric counterparts are the folium (superior semilunar lobule), tuber (inferior semilunar lobule), pyramid (biventral lobule), uvula (tonsil), and nodule (flocculus) allergy forecast league city discount 10 mg zyrtec free shipping. In the anatomic position, essentially the most inferior part of the inferior vermis is the pyramid. The most distinguished fissure on the suboccipital surface is the good horizontal fissure, which is a circumferential fissure that begins in the posterior cerebellar notch between the folium and the tuber and runs forward and slightly downward on the suboccipital floor, between the superior and inferior semilunar lobules, after which onto the petrosal surface as the petrosal fissure. After removal of the tonsils, the inferior portion of the roof of the fourth ventricle comes into view. After removing of the inferior portion of the roof of the fourth ventricle, the floor of the fourth ventricle is exposed. The floor of the fourth ventricle has a rhomboid form and consists of a strip between the lower margin of the cerebellar peduncles and the positioning of attachment of the tela choroidea; called the junctional part, this strip is shaped by the medullary striae, which prolong into the lateral recesses. The junctional half divides the ground of the fourth ventricle into two unequal triangles: the superior and larger one, with its apex directed towards the aqueduct, is the pontine part, and the inferior and smaller one, with its apex directed towards the obex, is the medullary part of the ground. These three parts of the ground are also divided longitudinally into two symmetrical halves by the median sulcus. The veins of the posterior fossa can be differentiated into the petrosal group, the superior or galenic group, and the posterior or tentorial group. The superior or galenic group consists of (1) the mesencephalic tributaries-the median anterior pontomesencephalic, lateral anterior pontomesencephalic, lateral pontomesencephalic, lateral mesencephalic, peduncular, posterior mesencephalic, and tectal veins-and (2) the cerebellar tributaries-the precentral cerebellar vein and its variants and the superior vermian vein. The posterior or tentorial group includes the inferior vermian vein and its superior and inferior retrotonsillar tributaries and the superior and inferior hemispheric veins. The lateral medullary phase programs beside the medulla and extends from the inferior olive to the origin of the glossopharyngeal, vagus, and accent nerves. The telovelotonsillar or supratonsillar segment programs in the cleft between the tela choroidea and the inferior medullary velum rostrally and the superior pole of the cerebellar tonsil caudally. The junction of the posterior medullary and supratonsillar segments known as the choroidal point. It programs posteriorly, laterally, and usually downward on the stomach of the pons, in contact with either the superior or inferior facet of the abducens nerve. In this course it supplies the lateral side of the lower two thirds of the pons and the higher medulla. Seventy-seven percent of inside auditory arteries and 49% of recurrent perforating arteries to the brainstem arise from this segment. The meatal segment is positioned within the vicinity of the internal auditory meatus, the place the nerve-related vessels flip towards the brainstem; this section often varieties a laterally convex loop, the meatal loop, directed toward or by way of the meatus. The postmeatal segment begins distal to the nerves and courses medially to provide the brainstem and the cerebellum. The caudomedial artery originates on the lateral aspect of the pons within the neighborhood of the sixth nerve and programs posterosuperiorly towards the pontomedullary sulcus; it has a caudal loop on the lateral aspect of the pons and medulla. This lateral loop can course on the anteroinferolateral facet of the flocculus or on the petrosal side of the biventral lobule. Multiple small arteries to the choroid plexus of the lateral recess typically arise from the inside aspect of this lateral loop. The superior cerebellar artery is probably the most rostral of the infratentorial vessels, and it arises near the apex of the basilar artery and encircles the pons and the decrease midbrain. It provides the tentorial floor of the cerebellum, the upper brainstem, the deep cerebellar nuclei, and the inferior colliculi. The anterior pontomesencephalic segment courses laterally underneath the oculomotor nerve on the anterior side of the upper pons, often in an arcuate convex curve inferiorly; the configuration of the anterior pontomesencephalic section is expounded to the peak of the basilar bifurcation. With a low basilar bifurcation (anterior to the pons), this phase tends to cross upward, whereas with a excessive basilar bifurcation (anterior to the midbrain), this section pursues an anterior and inferior course. The anterior a half of this phase is commonly visible above the free edge of the tentorium, whereas its caudal loop projects toward and sometimes reaches the foundation entry zone of the trigeminal nerve. The terminal portion of the vermian department curves around the tuber in the posterior cerebellar notch. Inside the cerebellomesencephalic fissure, the rostral and caudal trunks ship off small precentral branches. Finally, the cortical section is represented by the hemispheric and the vermian branches, which provide the tentorial surface of the cerebellum. It is an important arteriographic landmark for locating the anterolateral margin and the anterior angle of the cerebellum. At the lateral end of the internal acoustic meatus, the vertical Bill bar and the transverse crest divide the fundus of the meatus into four quadrants: the facial nerve is positioned within the anterosuperior quadrant, the cochlear nerve in the anteroinferior quadrant, the superior vestibular nerve within the posterosuperior quadrant, and the inferior vestibular nerve within the posteroinferior quadrant. Microsurgical anatomy of the choroidal arteries: fourth ventricle and cerebellopontine angles. Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve advanced. Mesial temporal lobe and its vascular relationship as utilized to amygdalohippocampectomy. Transchoroidal strategy to the third ventricle: an anatomic research of the choroidal fissure and its medical application. The insula and deep middle cerebral venous drainage system: regular anatomy and angiography. Microneurosurgery: Microsurgical Anatomy of the Basal Cisterns and Vessels of the Brain, vol 1. Miyashiro n James Eberwine Commenting on the construction and connections of neurons during his acceptance speech for the Nobel Prize in Medicine, Ramon y Cajal proposed that these fibres, ramifying a quantity of times, at all times proceed in the path of the neuronal body, or towards the protoplasmic expansions around which arise plexuses or very tightly sure and rich nerve nests [these] morphological constructions, whose form varies in accordance with the nerve centres being studied, affirm that the nerve components possess reciprocal relationships in contiguity however not in continuity. It is confirmed additionally that those kind of intimate contacts are at all times established, not between the nerve arborizations alone, however between these ramifications on the one hand, and the physique and protoplasmic processes on the other. With these observations in help of the neuron doctrine in 1906, so began one of the most abiding traces of scientific pursuit in biology-understanding the principal mechanisms by which the destiny of central neurons are specified throughout improvement at the correct time and place to facilitate the quadrillion synaptic connections that are established, maintained, and reworked. These arrays of neural networks codify our perceptions and other cognitive capabilities. To accomplish that, synapses bring collectively in apposition specialised morphologic buildings of the presynaptic, normally axonal, and postsynaptic, sometimes dendritic, subcellular neuronal domains often ensheathed by the end-feet of astrocytes. The precision and power of these connections depend on the pinpoint placement of gene products in every of these mobile compartments. Our understanding of neuroscience in these molecular phrases has been one of the fundamental challenges up to now a number of many years however has been difficult by the various intrinsic properties of neurons-including morphology, types of neurotransmitter release, projection targets, and fundamental input/ output characteristics-that exist along a wide spectrum of neuronal phenotypes even within the identical neuroanatomic region. Over the past a number of many years, neuroscientists have embraced a quickly evolving set of molecular biologic techniques to gain insight into understanding these dynamics of gene expression. These findings have been critical in understanding not only the mechanistic underpinnings of regular improvement but also the role that some genes play in neurological ailments from the developmental to the degenerative.
Zyrtec 10 mg discount without a prescription
Thus, the point prevalence of persistent painful peripheral polyneuropathy is on the order of 10�20% of patients with diabetes mellitus (Daousi et al 2004) allergy with fever cheap 10 mg zyrtec amex. In fact, it is among the challenges of the sphere to grasp the factors that decide why painful symptoms develop in some people solely with apparently identical conditions and what determines the range of the preliminary signs allergy medicine xy zyrtec 5 mg free shipping. Data from Gierthmuhlen J, Maier C, Baron R, et al 2012 Sensory signs in complex regional ache syndrome and peripheral nerve damage. Neuropathies characterized by fast degenerative change usually tend to be painful. The co-existence of degenerative and regenerative modifications seems to be an necessary issue (Brown et al 1976). Ischemia in nerves could exacerbate paresthesias and ache secondary to peripheral injury, and in sure circumstances, extreme ischemia, as in vasculitis, is the cause for neuropathies that might be very painful (Collins and Periquet 2004). Pain could also be evoked by excitation of the nervi nervorum in mononeuropathies or in sure polyneuropathies (Asbury and Fields 1984). Neuropathies involving small fibers, with or without largefiber involvement, are sometimes painful. Many research converge to counsel that axonal injury involving a portion of the nociceptive fibers in a peripheral nerve is the only most important causal factor for neuropathic pain: 1. There are several painless neuropathies in which smalldiameter sensory neurons are largely spared that strongly endorse this view. Thus, selective axonal or demyelinating lesions of motor fibers, as in motor neuron disease or multifocal motor neuropathy with conduction block, are usually painless. Finally, gain-of-function mutations in ion channels which might be prevalently expressed in nociceptors, such as Nav1. These experimental research in sufferers are entirely in settlement with the neuropathological observations talked about earlier that implicate small-diameter primary afferent fibers as the primary culprits in peripheral neuropathic ache: 1. Pain is usually abolished or no less than significantly reduced by local anesthetic block of broken peripheral nerves (Arn�r et al 1990, Fields et al 1997) or affected pores and skin (Gracely et al 1992, Rowbotham et al 1995), thus indicating that neural activity arising in the nerve or possibly even in the receptive endings contributes to the pain. Stimulus-independent ache and some types of stimulusinduced pain sensations persist throughout a differential nerve fiber block that eliminates conduction in myelinated nonnociceptive afferents (Campbell et al 1988, Ochs et al 1989, Ochoa and Yarnitsky 1993). Psychophysical experiments point out that the magnitude of ongoing ache correlates with the levels of nociceptor activity (Gracely et al 1992, Koltzenburg et al 1994). Microneurographic multiunit recording from the sural nerve in a patient with compression of the S1 spinal root by a herniated disc. A, Excitation of mechanosensitive units within the receptive field by tactile stimulation (bars). B, Straining- and chin�chest maneuver�provoked paresthesias and ectopic discharge of afferent fibers originating from the compressed root. Abnormal ectopic activity in myelinated mechanosensitive fibers has been recorded in patients with traumatic nerve lesions, entrapment neuropathies, and radiculopathies. A traditional research by Nystr�m and Hagbarth (1981) provided evidence that ectopic excitation can occur at a number of websites in broken sensory neurons. Ongoing activity and mechanical sensitivity were recorded proximal to a nerve neuroma in an amputee with phantom limb pain. Microneurographic studies of unmyelinated nociceptors in sufferers with polyneuropathy have proven that individuals with pain have a significantly larger share of ongoing activity than do these without ache (Kleggetveit 2012). This distinction was particularly pronounced within the inhabitants of mechanically insensitive nociceptors, which are regarded as important for central sensitization. This irregular spiking with pure stimulation supplies an evidence for the hyperalgesia in these sufferers. Abnormal nociceptors have additionally been recorded in patients affected by erythermalgia (also known as erythromelalgia), a situation characterised by painful, red, scorching extremities. The inherited type is attributable to a gain-of-function mutation within the gene encoding the voltage-gated sodium channel Nav1. In heterologous expression systems the mutations can produce a hyperpolarizing shift in activation and a slowing of deactivation (Cummins et al 2004). Stimulus-Induced Pain (Hyperalgesia) Stimulus-induced ache is widespread in individuals with neuropathic pain. Most typically sufferers report mechanical hyperalgesia followed by hyperalgesia to heat and cold. In neuropathic circumstances the excellence between primary and secondary areas is much less clearly defined than within the traditional research on tissue harm but in all probability corresponds to the tissue supplied by broken nerves and the realm outside this innervation territory. Hyperalgesia to Heat Hyperalgesia to warmth is a trademark of tissue damage, and this symptom happens solely sometimes in neuropathic situations. The hyperalgesia to warmth persists during differential nerve blocks of myelinated fibers, and microneurographic investigations have demonstrated chronic sensitization of nociceptors to heat (Cline et al 1989, Torebj�rk 1990). Sensitization to Catecholamines Sensitization of nociceptors may prevail in sympathetically maintained pain, and though no onerous epidemiological information can be found, the number of sufferers with a predominant sympathetically maintained component of their ache is probably 932 A Section Seven Clinical States/Neuropathic Pain Before block After block had provided ache aid, intracutaneous injection of adrenoceptor agonists can beneath sure circumstances rekindle the ongoing pain and hyperalgesia (Davis et al 1991, Torebj�rk et al 1995). Furthermore, injections of catecholamines around a stump neuroma can precipitate attacks of ache in people (Chabal et al 1992). Since noradrenalin-induced pain occurs throughout a differential blockade of myelinated fibers, unmyelinated fibers seem to signal sympathetically maintained ache (Torebj�rk et al 1995). This has been corroborated by direct microneurographic recordings of C fibers in a affected person with sympathetically maintained pain, in whom activation of sympathetic efferents or injection of noradrenaline led to excitation of mechanically insensitive nociceptors (J�rum 2007). Mechanical Hyperalgesia the signs and signs of mechanical hyperalgesia in neuropathy are numerous, and no less than three distinct varieties have been described in sufferers with neuropathic ache: (1) brushevoked ache, (2) pinprick hyperalgesia, and (3) hyperalgesia to blunt strain (Koltzenburg 1996). There is consensus that the touchevoked ache in neuropathic conditions is signaled out of the skin by sensitive mechanoreceptors with giant myelinated axons that normally encode non-painful tactile events (see Table 65-2). First, differential blockade of huge myelinated non-nociceptive afferents abolishes brush-evoked pain (Campbell et al 1988, Gracely et al 1992, Koltzenburg et al 1994). Second, electrical stimulation (Price et al 1989, Torebj�rk 1990) of those afferents causes painful dysesthesias. Third, reaction time measurements point out that brushevoked ache is signaled by fast conducting myelinated fibers (Fruhstorfer and Lindblom 1984). Finally, light punctate mechanical stimuli that may activate solely sensitive mechanoreceptors are sometimes referred to as painful in patients with neuralgia (Price et al 1992, Koltzenburg et al 1994). Hyperalgesia to pinprick stimuli- sometimes elicited by probing the pores and skin with a stiff von Frey hair-can be found in sufferers suffering from neuropathy (Pappagallo et al 2000). Hyperalgesia to blunt pressure has also been described in sufferers with neuropathic pain (Ochs et al 1989, Price et al 1992, Ochoa and Yarnitsky 1993), and differential nerve block experiments counsel that this type of hyperalgesia is signaled by nociceptors in people. Microneurographic multi-unit recording from a pores and skin fascicle of the median nerve on the wrist in a patient with a hand amputation and phantom pain in the hand and fingers that was accentuated by taps on a stump neuroma. This response (arrow) was eradicated by the local anesthetic block (right), which also abolished tap-induced accentuation of the phantom pain. The importance of the sympathetic nervous system in the technology of pain has been the primary target of a long, if controversial, debate.
Diseases
- Harrod Doman Keele syndrome
- Empty sella syndrome
- Symphalangism, distal, with microdontia, dental pulp stones, and narrowed zygomatic arch
- Taeniasis
- Pulmonary surfactant protein B, deficiency of
- Environment associated hypertension
Zyrtec 10 mg discount on line
One explanation for painless myocardial ischemia is "neural stunning," whereby earlier ischemic activity renders the sensory sympathetic fibers much less delicate (Pettersen et al 1995, Abe et al 1998) seasonal allergy symptoms quiz quality zyrtec 5 mg. Another chance is that cardiac afferents are normally rather unresponsive and sensitized solely by pathology, extra so in some than others (Malliani 1986) allergy testing edinburgh generic 5 mg zyrtec free shipping. Approximately 20% of sufferers in whom coronary artery illness is suspected clinically are found to have regular to nearly normal coronary arteries on the time of angiography (Kemp et al 1986), and some proportion of these sufferers are stated to have cardiac syndrome X (Shimokawa and Yasuda 2008, Cannon 2009, Lim et al 2009). Although the definition of this syndrome continues to evolve (Vermeltfoort et al 2010), it reasonably consists of exertional angina pectoris accompanied by ischemia-like modifications on the electrocardiogram or reversible perfusion deficits with stress testing regardless of normal findings on coronary arteriography. Patients with cardiac syndrome X are extra doubtless to be women, particularly those that are post-menopausal (Kaski 2002) and have estrogen deficiency (Rosano et al 1995, Kaski 2006). Patients with cardiac syndrome X usually have a tendency to report pain with mechanical or benign electrical stimulation of the heart, intracoronary injection of contrast media, and infusion of adenosine or dipyridamole (Shapiro et al 1988, Cannon et al 1990b, Lagerqvist et al 1992, Rosen et al 1994b, Pasceri et al 1998), and this sensitivity additionally happens with esophageal stimulation (Cannon et al 1990a). Anxiety and panic dysfunction are sometimes noticed in sufferers with cardiac syndrome X (Bass et al 1983, Beitman et al 1989, Pasceri et al 1998, Rutledge et al 2001). Functional brain imaging reveals a stage of central activation in syndrome X patients comparable to that noticed in those with myocardial ischemia, however with characteristic activation of the insular cortex (Rosen and Camici 2000, Rosen et al 2002). Microvascular abnormalities because of coronary endothelial dysfunction look like an necessary part of cardiac syndrome 726 Section Five Clinical States/Viscera X (Hurst et al 2006). Long-term consequence research of patients with cardiac syndrome X initially revealed little influence on survival however demonstrated how unresolved chest pain may impair way of life (Kaski et al 1995, Lichtlen et al 1995). However, newer data acknowledge that coronary and cerebrovascular illness is extra likely to develop in these with demonstrable endothelial dysfunction (Targonski et al 2003, Bugiardini et al 2004). Pericardium A massive number of idiopathic, inflammatory, neoplastic, congenital, metabolic, traumatic, rheumatological, iatrogenic, and infectious circumstances, either systemic or specifically associated with the pericardium or adjoining organs, can lead to ache of pericardial origin (Spodick 2001). Pericardial ache could be severe, is often sudden in onset and substernal in location with radiation similar to that of myocardial ischemia however may also include the trapezius ridge, and can be sharp or boring in character. It worsens with inspiration and recumbency but improves with sitting and leaning forward. Auscultation could reveal a rub with components related to atrial systole, ventricular systole, and diastole. Pericardial fluid might render coronary heart sounds more distant, and constriction could introduce a sound in early diastole. Fever could also be present together with hemodynamic alterations related to pericardial effusion or constriction. For each acute and chronic pericardial disease, ache is generally much less of a difficulty than management of the underlying condition and the physiology that may accompany constrictive pericarditis or the tamponade produced by pericardial effusion (Sparano and Ward 2011). However, ache can turn into a dominant characteristic of recurrent (Fowler 1990) and persistent pericarditis (Gutman and Haft 1979). Great Vessels Although the pain related to aortic dissection is well known, other kinds of aortic pathologies can lead to pain of aortic origin which will also masquerade as pain arising from another organ system. The medical findings in sufferers with aortic dissection may be "diverse" (Hagan et al 2000), with the pain being described as an acute onset of extreme sharp pulsatile ache that often migrates along the course of the dissection. Anterior chest pain radiating to the jaw and neck is related to dissection of the ascending aorta, whereas ache within the again, stomach, and decrease extremities is related to dissection of the descending aorta (Spittell et al 1993, Hagan et al 2000). A sudden onset of intense pain may also signal acute enlargement or rupture of an current aneurysm. Myocardial ischemia from co-existing coronary artery disease or from cardiac involvement of an ascending dissection may be present. Inflammatory and autoimmune disease also can produce pain of aortic origin (Wooley et al 1998) that can turn into chronic (Slobodin et al 2008). Venous obstruction of any etiology can result in epidural venous engorgement and radiculopathy (Paksoy and Gormus 2004). Lungs, Diaphragm, and Tracheobronchial Tree Although painless dyspnea is often the one symptom of pulmonary embolism, ache thought to sign pulmonary infarction happens in about half of sufferers (Goldhaber et al 1999). Pleuritic ache is experienced when smaller emboli lodge within the distal arterial tree adjacent to the pleura and must be differentiated from more benign causes of pleuritic pain (Branch and McNeil 1983). Distention of pulmonary artery mechanoreceptors (Nishi et al 1977), as can also occur with pulmonary hypertension, may likewise produce discomfort (Brims et al 2010). The prognosis of pulmonary embolism begins with suspicion, is aided by a quantity of medical decision-making guidelines (see Table 52-3) and checks, and is related to a 3-month mortality of 15% (Goldhaber et al 1999). Malignant, infectious, inflammatory, and autoimmune processes of the lung and pleura can result in pain and secondary pleural effusions (Brims et al 2010). Pain arising from pleural illness is regularly anginal in high quality and could also be tough to treat when the underlying condition is chronic (Law et al 1984, Mukherjee et al 2000). Pain associated to the pleura generally arises from the parietal pleura, though lesions along the interlobular fissures of the lungs look like capable of producing pain (England et al 1989, Rusch 1990, Mukherjee et al 2000). The location of the pleuritic pain can usually present some extent of localization of the underlying pulmonary processes. The analysis of pneumonia may be difficult to make however could be aided by a number of scientific choice rules (see Table 52-3). The clinical spectrum of cough, fever, sputum manufacturing, and leukocytosis is accompanied by pleuritic chest pain almost half the time (Fine et al 1999). The absence of pleuritic pain in many patients most likely represents an absence of peripheral parenchymal involvement. Consistent with this, parapneumonic effusions will develop in roughly 40% of sufferers (Koegelenberg et al 2008). The pleuritic pain accompanying pneumonia can persist; it lasts at least 30 days in 13% of patients with pneumococcal pneumonia (Brandenburg et al 2000). Ipsilateral pleuritic chest ache accompanies spontaneous pneumothorax in 90�100% of instances (Seremetis 1970, Wilcox et al 1995). The explanation for this ache has not but been established, however some research indicate that pleural inflammation happens with pneumothorax (Kalomenidis et al 2005, 2008). Pain is skilled by two-thirds of those with spontaneous pneumomediastinum (Iyer et al 2009). Dyspnea, cough, and hiccups are disagreeable signs that originate within the thorax and regularly sign the presence of underlying pathology but can, themselves, turn into disabling and require intervention (Jacobs 2003). Although the definition of dyspnea has not been standardized, it includes air hunger, elevated work or effort of respiratory, and chest tightness (Burki and Lee 2010, Nishino 2011). Refractory dyspnea is usually a part of advanced pulmonary disease, coronary heart failure, and most cancers, with 28% of sufferers reporting dyspnea of a minimum of reasonable depth throughout their ultimate 6 weeks of life (Reuben and Mor 1986, Ripamonti et al 1998; see Chapter 76). Hiccups are frequently encountered in palliative care (Jacobs 2003, Schuchmann and Browne 2007) but can even sign myocardial ischemia (Krysiak et al 2008), pulmonary embolism (Zylicz 2010), aortic aneurysm (Samuel 1952), brain stem tumors (Fischer and McLean 1982), and other problems (Howard 1992). It can persist for minutes to hours and might worsen postprandially, within the supine place, and with emotional stress. As with typical anginal pain, the symptoms of heartburn and regurgitation can be brought on by heavy train similar to treadmill testing. The presence of acid could sensitize the esophagus to mechanical stimulation (Hu et al 2000). The presence of acid within the lower part of the esophagus can lower the pain threshold of the upper part of the esophagus and chest wall in regular people and to a greater extent in these with non-cardiac chest ache whose pain threshold was already low to start with (Sarkar et al 2000). Those who experience anginal ache with esophageal acid infusion also have proof of altered cardiac autonomic perform (Tougas et al 2001).

Zyrtec 10 mg quality
Painful Diagnostic and Therapeutic Procedures Needle procedures are a serious source of distress for kids with most cancers (Zeltzer et al 1989) allergy treatment 5mm discount 5 mg zyrtec free shipping. Common procedures embrace venipuncture, venous cannulation, lumbar puncture, bone marrow aspirate and biopsy, and removal of central venous lines allergy symptoms guinea pig buy zyrtec 10 mg with visa. It is crucial to deal with the pain and distress related to the preliminary diagnostic procedures very successfully. Children want adequate preparation before needle procedures to reduce their fear and nervousness. Effective preliminary treatment will set a pattern of trust and confidence for patients and families. Conversely, if the primary bone marrow aspiration or lumbar puncture is a horrific experience, there will be a carryover impact of persistent worry and distress to future procedures. A randomized controlled trial compared a technique of rapid opioid delivery-oral Box 74-1 Commonsense however Frequently Forgotten Aspects of Pediatric Procedures � Minimize pointless procedures, especially repeated venipuncture. Get all supplies and gear prepared beforehand in order that the process is accomplished as rapidly as possible. Topical cooling with ice or fluorocarbon coolant sprays has been used with some success (Abbott and Fowler-Kerry 1995). Iontophoresis includes the utilization of an electrical present to accelerate penetration of the drug through the pores and skin. Iontophoresis can produce skin analgesia rapidly and with good depth of penetration (Zeltzer et al 1991). There are a quantity of ongoing approaches to enhance the efficacy and cut back the time of onset for non�needle-based strategies of cutaneous anesthesia. Both local heating (Shomaker et al 2000) and ultrasound (Katz et al 2004) can dramatically accelerate the onset of topical local anesthetic formulations. Local anesthetic infiltration can scale back the pain that occurs with deeper needle procedures. Prior use of topical anesthesia can cut back the discomfort of the infiltrating needle. The pain of infiltration may be lowered by neutralizing commercially provided acidic local anesthetic options instantly earlier than use with sodium bicarbonate in the following ratios: 1 half sodium bicarbonate (8. Conscious sedation refers to the administration of anxiolytics and analgesics to render the child sedated and comfortable however nonetheless in a position to answer stimuli and preserve airway reflexes and air flow. For each acutely aware sedation and common anesthesia, protected practice necessitates administration by practitioners with expertise in airway administration and with information of the relevant pharmacology and medical issues. Protocols for monitoring and drug dosing can help reduce danger (Hoffman et al 2002). Pure sedatives, similar to pentobarbital, chloral hydrate, and midazolam, are extensively used for painless procedures that require immobility, similar to radiation therapy. The combination of midazolam with either fentanyl or low-dose ketamine is usually secure and efficient (Frank et al 1988, Marx et al 1997, Parker et al 1997). The intravenous route is helpful due to rapid 1063 onset, full bioavailability, and the flexibility to titrate incremental doses to impact. Ketamine has obtained widespread use as a outcome of it produces analgesia, dissociation, and secure respiration in most youngsters. Although respiration is mostly nicely maintained, maybe higher than with opioids dosed to comparable impact, ketamine has the drawback of no pharmacological reversal agent, and issues of respiratory depression have been reported (Mitchell et al 1996, Green and Rothrock 1997, Litman 1997, Roelofse and Roelofse 1997). Ketamine should be used primarily in a setting the place personnel with advanced airway expertise are available. The incidence of dysphoria, unhealthy dreams, or prolonged sedation remains in dispute (Valentin and Bech 1996). Oral benzodiazepine�opioid or benzodiazepine� ketamine mixtures could be efficient, though absorption varies and oral�parenteral ratios are solely approximations (Hollman and Perloff 1995, Qureshi et al 1995). If oral sedation is used, adequate time should elapse to achieve the height drug impact. Because of variability in onset and offset, kids must be noticed for the event of deep sedation or respiratory despair. Some kids will turn out to be stressed or attempt to stand up and walk and will injure themselves if unattended. Oral�transmucosal fentanyl has speedy absorption and good efficacy for bone marrow aspiration and lumbar Box 74-2 Recommendations for Conscious Sedation in Children � Establish protocols, education programs, and an evaluation program to trace efficacy and complications. Bone marrow aspiration is a supply of severe distress in youngsters (Katz et al 1980, Jay et al 1983). Guided imagery, leisure, hypnosis, aware sedation, and basic anesthesia have been shown to be effective modalities for lowering misery in this setting (Jay et al 1983, 1987, 1995). Removal of Central Venous Lines Tunneled central venous lines require removing, both electively when therapy programs are completed or extra urgently in cases of an infection or occlusion. Brief basic anesthesia and aware sedation are widely used for these procedures. For instance, a 12-year-old who is a superb hypnotic topic and who experiences extreme nausea or dysphoria with sedation or general anesthesia might favor hypnosis over pharmacological measures. Conversely, a 3-year-old who has had severely traumatic experiences with previous procedures might do higher with a brief basic anesthetic. Pharmacological and psychological approaches ought to be seen as complementary, not mutually unique. Nitrous oxide 30�50% in oxygen can be utilized for sedation (Gamis et al 1989, Bouffet et al 1996) with good security, rapid onset and offset, no requirement for intravenous entry, and good analgesia. Some children will resist the masks, will report bothersome desires (particularly with concentrations in extra of 50%), or will discover nitrous oxide insufficient for portions of extra painful procedures. Combining nitrous oxide with different sedatives or analgesics requires expertise; responses differ significantly (Litman et al 1996). The growth of shorter-duration basic anesthetic agents has greatly facilitated these procedures, each in operating room areas and in distant places. If intravenous access is available, propofol is broadly favored due to its rapid onset, speedy pleasant emergence, and antiemetic results (Vangerven et al 1992, Frankville et al 1993). If inhalational anesthesia is required, the vapor anesthetic sevoflurane has turn into well-liked due to its candy odor and intensely speedy onset and offset. Some youngsters worry the masks or dislike the pungent aroma of unstable anesthetics, particularly halothane and isoflurane (Jay et al 1995). There is considerable controversy regarding the relative dangers and benefits of transient deep sedation or basic anesthesia provided by anesthetists (Maunuksela et al 1986) versus aware sedation supplied by non-specialists (Cote 1994, Maxwell and Yaster 1996). Many pediatric facilities use a twotiered approach, with aware sedation for sure procedures performed by oncologists and other non-anesthetists in accordance with protocol guidelines and with a sedation service staffed by pediatric anesthetists for higher-risk patients, for more intensive or demanding procedures, or in instances of failed sedation by non-anesthetists (Gozal et al 2004). Lumbar Puncture the misery of lumbar puncture is related in part to the required body position and the need to remain still, as nicely as pain from contact of the needle with skin, bony spinous processes, or laminae.
Zyrtec 10 mg discount free shipping
The reported proportion of such afferents among the many total organ afferent innervation in rodents ranges widely (3�27%) however is generally a small fraction of the visceral innervation allergy shots ottawa 10 mg zyrtec buy with amex. Their position in cross-organ sensitization (see below) stays to be confirmed as being functionally vital allergy forecast edmonton alberta zyrtec 5 mg without prescription. Accordingly, the diffuse character and poor localization of visceral ache are contributed to by the widespread intraspinal arborization of visceral afferent terminals and by somatovisceral and viscerovisceral convergence onto second-order spinal neurons, thus challenging patients and physicians alike to simply establish the source or sources of visceral pain. Neurochemistry of Visceral Primary Afferents As indicated above, most visceral receptive endings in organs are sometimes non-encapsulated ("free") and associated with slowly conducting unmyelinated (C) or thinly myelinated (A) axons of usually small- to medium-diameter somata in the dorsal root and nodose ganglia. It could be handy and helpful if neuronal operate might be assigned on the basis of cell measurement and myelination, but neither characteristic defines a nociceptor (Gold and Gebhart 2010). Beyond cell dimension, cell content has been used to broadly segregate nociceptive afferents into peptidergic and non-peptidergic (Snider and McMahon 1998). Even this classification, nevertheless, obscures differences between nociceptors innervating different tissues. These further markers also have limitations, principally that their distribution or presence varies amongst subpopulations of nociceptors defined by the target of innervation, which moreover adjustments as the state of the tissue changes. This fraction increases additional during inflammatory processes associated with ache. Not surprisingly, there also are vital differences in cell content material markers between the two innervations of the identical organ. Mucosal noxae can thus lead to vasodilatation and hyperemia, inflammatory infiltration via chemotaxis, capillary leakage with exudate of plasma and swelling, and activation of smooth muscle cells, as well as increased secretion in epithelial cells, all of that are features usually related to neurogenic irritation. Emerging evidence suggests that this mechanism contributes to the pathogenesis of acute and persistent diseases involving the viscera. Gallbladder, esophageal, urinary bladder, and colon distention typically excites visceroceptive spinal neurons but also can inhibit the continued activity of some. Most visceroceptive spinal neurons excited by distending stimuli have low thresholds for response in the physiological vary. Importantly, visceroceptive spinal neurons excited by distention encode the distending stimulus all through the range of distending pressures examined. Because these visceroceptive spinal neurons may be antidromically invaded from the thalamus, nucleus gracilis (post-synaptic dorsal column neurons), or rostral spinal wire, the enter received is conveyed to supraspinal websites and thus contributes to pseudo-affective reflexes, in addition to to conscious appreciation of visceral input. Visceroceptive spinal neurons inhibited by organ distention are probably concerned in local or short-loop reflexes. As indicated above, convergence of afferent input is attribute of visceroceptive spinal neurons. Virtually all visceroceptive spinal neurons obtain convergent somatic enter, if not also convergent input from other viscera. Consistent with their capability to encode visceral stimulus intensity into the noxious range, sufficient excitatory convergent somatic input (commonly from skin) is usually noxious. A, Mean responses, illustrated as histograms (1-second bin width), of spinal neurons to a noxious depth of colorectal distention (80 mm Hg). All neuron varieties reply at short latency to distention, however only neuron sort 1 is tightly linked to stimulus period. Neuron kind 2 exhibits a sustained afterdischarge, and the inhibitory effect of distention is lengthy lasting as properly. Neuron varieties 1 and 2 are additional characterised in B, the place normalized stimulus�response functions are illustrated. Type 2 however not type 1 neurons become sensitized after colon inflammation (see Traub 2007). It is often the case that visceroceptive spinal neurons with a high threshold for response to distending stimuli are nociceptive specific�like with respect to their cutaneous input. It is rare for visceroceptive neurons to reply solely to non-noxious enter from the convergent cutaneous receptive area. Studies comparing visceral and somatic stimulation reveal refined differences (Dunckley et al 2005a) that largely correlate with the more important emotional impact skilled during visceral ache. For instance, sufferers with irritable bowel syndrome exhibit increased areas of referred sensation and report discomfort and tenderness on abdominal palpation. Because visceroceptive spinal neurons with thresholds for response higher than 20 mm Hg are predominantly excited by noxious convergent cutaneous enter, sometimes exhibit sustained responses to organ distention that persist after termination of the stimulus, project to supraspinal sites, and become sensitized after organ insult, they look like the population of visceroceptive spinal neurons most essential for spinal visceral nociceptive processing with respect to each acute visceral ache and visceral hypersensitivity. Additional studies have demonstrated that post-synaptic spinal neurons originating primarily in lamina X ascend the dorsal columns to the thalamus through cuneothalamic pathways. Consistent with the importance of this pathway, transection of the dorsal columns abolished nocifensive habits in response to noxious visceral stimulation. Within the thalamus, the primary relay station for somatosensory enter, visceral afferent input primarily tasks into the ventral posterolateral nucleus, the place once more many of the neurons obtain convergent somatic input. Studies of mind activation utilizing positron emission tomography or functional magnetic resonance imaging have recognized websites of cortical pain processing in people. Hollow-organ balloon distention is an adequate noxious stimulus and easy to control in period and intensity. It is relevant for use in non-human animal research because distention of hollow organs in humans reproduces the distribution of referred sensations from a viscus, as properly as the standard and depth of the visceral sensation (Ness and Gebhart 1990). Chemical and thermal stimuli are less nicely characterised behaviorally, though visceral chemonociception is a rising space of investigation. With our rising understanding of nociceptor activation, specific agonists have been used to activate visceral nociceptive pathways. Functional Properties of Visceral Mechanoreceptors (in Vivo) When distention of hollow organs has been used because the stimulus, two teams of mechanosensitive afferent fibers have been present in spinal visceral nerves. The larger proportion, usually 75�80% of the pattern, respond at low distending pressure in the physiological vary. The view that low- and highthreshold mechanoreceptors in the viscera are the counterpart of somatic non-nociceptors. These features of visceral afferent fiber innervation could explain why normally subliminal physiological stimuli are perceived as uncomfortable or painful in individuals with practical bowel and bladder issues. With respect to mechanosensitive vagal afferent fibers, solely a single inhabitants of fibers with low thresholds for response to gastric distention has been described in vivo, although response magnitude continues to increase nicely into the noxious range of distention. Though characterised as mechanoreceptive, each vagal afferent fibers and spinal visceral afferent fibers (Box 51-1) are generally multimodal and reply to thermal and/or chemical stimuli, in addition to balloon distention. Furthermore, publicity to either thermal (heat) or chemical stimuli sometimes sensitizes subsequent responses to organ distention, as does organ insult. Although not established for all mechanosensitive fibers, it appears that all spinal and vagal mechanosensitive fibers studied in vivo reply to no less than two modalities of stimuli. Functional Properties of Visceral Mechanoreceptors (in Vitro) More just lately, in vitro organ�nerve preparations have permitted broader practical characterization of mechanoreceptive endings within the colon, esophagus, abdomen, ureter, urinary bladder, and uterus. Mucosal, rigidity (muscular), and muscular�mucosal receptors have been characterised within the vagal afferent innervation of the esophagus and stomach, and mesenteric, serosal, mucosal, muscular, and mucosal�muscular receptors have been described in the urinary bladder and colon. Mucosal�muscular receptors respond to light mucosal/ urothelial stroking, as well as to circumferential stretch. Mesenteric mechanoreceptors respond in a graded manner to von Frey�like probing along the mesenteric attachment, typically related to the vasculature but to not stretch. Although we are inclined to focus on endings in organs associated with mucosa, muscle, or serosal layers, axons of visceral sensory neurons on intramural blood vessels can also function transduction websites for mechanosensation, including responses to stretch and distention of hollow viscera. Use of the in vitro organ�nerve preparation has established that some vagal and a few spinal afferent fibers have a quantity of receptive fields within the stomach and colon, respectively, but testing typically reveals punctate receptive fields with diameters of 1�2 mm2.
Syndromes
- Whether there is any change in consciousness
- The person has a fever over 102 °F.
- Rape may occur between members of the same sex. This is more common in places such as prisons, military settings, and single-sex schools.
- Malnutrition
- Wheezing
- Severe pain or burning in the nose, eyes, ears, lips, or tongue
- Allergic reactions
- Breathing in (inhaling) a carbon dioxide-oxygen mixture. This treatment causes the arteries of the retina to widen (dilate).
- Dry mouth
- Name of the plant, if known

Buy zyrtec 10 mg cheap
Liu J, Jia H, Yang Y, et al: Cerebrospinal fluid cytology and scientific evaluation of 34 cases with leptomeningeal carcinomatosis, Journal of International Medical Research 37:1913�1920, 2009 allergy symptoms yahoo zyrtec 10 mg discount otc. Lossos A, Siegal T: Numb chin syndrome in most cancers sufferers: etiology, response to therapy, and prognostic significance, Neurology 42:1181� 1184, 1992 allergy treatment in kids zyrtec 5 mg cheap fast delivery. Malhotra N, Sumana G, Singh A, et al: Rupture of a malignant ovarian tumor in being pregnant presenting as acute abdomen, Archives of Gynecology and Obstetrics 281:959�961, 2010. Marangoni C, Lacerenza M, Formaglio F, et al: Sensory dysfunction of the chest as presenting symptom of lung most cancers, Journal of Neurology, Neurosurgery, and Psychiatry fifty six:1033�1034, 1993. Marini P, Vilgrain V, Belghiti J: Management of spontaneous rupture of liver tumours, Digestive Surgery 19:109�113, 2002. Marino C, Zoppi M, Morelli F, et al: Pain in early most cancers of the lungs, Pain 27:57�62, 1986. Markman M, Kennedy A, Webster K, et al: Use of low-dose oral prednisone to prevent paclitaxel-induced arthralgias and myalgias, Gynecologic Oncology 72:100�101, 1999. Martin R, Jourdain S, Clairoux M, et al: Duration of decubitus place after epidural blood patch, Canadian Journal of Anaesthesia forty one:23�25, 1994. Martinez-Lavin M: Hypertrophic osteoarthropathy, Current Opinion in Rheumatology 9:83�86, 1997. Matsumura Y, Akaza H, Isaka S, et al: the 4th research of prophylactic intravesical chemotherapy with Adriamycin in the remedy of superficial bladder cancer: the expertise of the Japanese Urological Cancer Research Group for Adriamycin, Cancer Chemotherapy and Pharmacology 30(Suppl):S10� S14, 1992. Maunsell E, Brisson J, Deschenes L: Arm problems and psychological distress after surgery for breast cancer, Canadian Journal of Surgery 36:315�320, 1993. Nikolajsen L, Ilkjaer S, Kroner K, et al: the affect of preamputation pain on postamputation stump and phantom pain, Pain seventy two:393�405, 1997b. Oki Y, Koike H, Iijima M, et al: Ataxic vs painful form of paraneoplastic neuropathy, Neurology sixty nine:564�572, 2007. Ollivier L, Gerber S, Vanel D, et al: Improving the interpretation of bone marrow imaging in most cancers patients, Cancer Imaging 6:194�198, 2006. Olsson H, Alm P, Kristoffersson U, et al: Hypophyseal tumor and gynecomastia previous bilateral breast cancer development in a person, Cancer 53:1974�1977, 1984. Ovesen P, Kroner K, Ornsholt J, et al: Phantom-related phenomena after rectal amputation: prevalence and clinical traits, Pain 44:289�291, 1991. Payer M: Neurological manifestation of sacral tumors, Neurosurgical Focus 15(2):E1, 2003. Miyamoto M, Sudo T, Kuyama T: Spontaneous rupture of hepatocellular carcinoma: a evaluation of 172 Japanese circumstances, American Journal of Gastroenterology 86:67�71, 1991. Naumann C, Erdine S, Koulousaki A, et al: Drug adverse occasions and system issues of intrathecal opioid supply for pain: origins, detection, manifestations, and management, Neuromodulation 2:92�107, 1999. Nguyen S, Hojjati M: Review of present therapies for secondary hypertrophic pulmonary osteoarthropathy, Clinical Rheumatology 30:7�13, 2011. Pilatrino C, Cilloni D, Messa E, et al: Increase in platelet rely in older, poorrisk sufferers with acute myeloid leukemia or myelodysplastic syndrome handled with valproic acid and all-trans retinoic acid, Cancer 104:101�109, 2005. Radiography and bone scintigraphy within the symptomatic and asymptomatic spine, Cancer sixty four:2207�2213, 1989. Postoperative ache undertreated within the United States, Journal of Pain & Palliative Care Pharmacotherapy 22:92�93, 2008. Prandoni P, Piccioli A: Thrombosis as a harbinger of cancer, Current Opinion in Hematology thirteen:362�365, 2006. Prasad D, Schiff D: Malignant spinal-cord compression, Lancet Oncology 6:15�24, 2005. Puel V, Caudry M, Le Metayer P, et al: Superior vena cava thrombosis related to catheter malposition in most cancers chemotherapy given via implanted ports, Cancer seventy two:2248�2252, 1993. Rajagopal A, Ramasamy R, Martin J, et al: Acute myeloid leukemia presenting as splenic rupture, Journal of the Association of Physicians of India 50:1435�1437, 2002. Rosenthal S, Kaufman S: Vincristine neurotoxicity, Annals of Internal Medicine 80:733�737, 1974. Russo P: Urologic emergencies within the most cancers patient, Seminars in Oncology 27:284�298, 2000. Scalone S, Sorio R, Bortolussi R, et al: Vinorelbine-induced acute reversible peripheral neuropathy in a patient with ovarian carcinoma pretreated with carboplatin and paclitaxel, Acta Oncologica forty three:209�211, 2004. Schonenberg P, Bastid C, Guedes J, et al: Percutaneous echography�guided alcohol block of the celiac plexus as remedy of painful syndromes of the upper stomach: examine of 21 cases, Schweizerische Medizinische Wochenschrift 121:528�531, 1991. Stillman M: Perineal pain: analysis and management, with specific consideration to perineal pain of most cancers. Suwanwela N, Phanthumchinda K, Kaoropthum S: Headache in mind tumor: a cross-sectional examine, Headache 34:435�438, 1994. Suzuma T, Sakurai T, Yoshimura G, et al: Pamidronate-induced remission of ache associated with hypertrophic pulmonary osteoarthropathy in chemoendocrine therapy�refractory inoperable metastatic breast carcinoma, Anticancer Drugs 12:731�734, 2001. Taillibert S, Laigle-Donadey F, Chodkiewicz C, et al: Leptomeningeal metastases from solid malignancy: a evaluation, Journal of Neuro-Oncology seventy five:85�99, 2005. Tardy B, Moulin N, Mismetti P, et al: Intravenous thrombolytic remedy in sufferers with phlegmasia caerulea dolens, Haematologica ninety one:281�282, 2006. Tasmuth T, von Smitten K, Hietanen P, et al: Pain and other signs after completely different treatment modalities of breast cancer, Annals of Oncology 6:453�459, 1995. Tasmuth T, von Smitten K, Kalso E: Pain and other signs during the first yr after radical and conservative surgery for breast cancer, British Journal of Cancer seventy four:2024�2031, 1996. Tharion G, Bhattacharji S: Malignant secondary deposit within the iliac crest masquerading as meralgia paresthetica, Archives of Physical Medicine and Rehabilitation seventy eight:1010�1011, 1997. Schulze T, Mucke J, Markwardt J, et al: Long-term morbidity of sufferers with early breast cancer after sentinel lymph node biopsy compared to axillary lymph node dissection, Journal of Surgical Oncology 93:109�119, 2006. Scully C, Epstein J, Sonis S: Oral mucositis: a challenging complication of radiotherapy, chemotherapy, and radiochemotherapy. Siegal T: Muscle cramps within the cancer patient: causes and treatment, Journal of Pain and Symptom Management 6:84�91, 1991. Skriapas K, Konstandinidis C, Samarinas M, et al: Pain stage and anal discomfort throughout transrectal ultrasound for guided prostate biopsy. Does intrarectal administration of local anesthetic earlier than periprostatic anesthesia makes any difference Sozzi G, Marotta P, Piatti L: Vagoglossopharyngeal neuralgia with syncope in the midst of carcinomatous meningitis, Italian Journal of the Neurological Sciences eight:271�275, 1987. A evaluation of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential as a radioprotector and cytotoxic chemoprotector, Drugs 50:1001�1031, 1995. Treasure T: Hypertrophic pulmonary osteoarthropathy and the vagus nerve: an historical notice, Journal of the Royal Society of Medicine 99:388�390, 2006. Twycross R, Harcourt J, Bergl S: A survey of pain in sufferers with advanced cancer, Journal of Pain and Symptom Management 12:273�282, 1996. Ulubas B, Ozcan C, Acka G, et al: Clivus metastasis of squamous cell carcinoma: a rare location, Journal of Clinical Neuroscience 12:97�98, 2005. Venturini M, Del Mastro L, Aitini E, et al: Dose-dense adjuvant chemotherapy in early breast cancer patients: results from a randomized trial, Journal of the National Cancer Institute 97:1724�1733, 2005. Virik K, Karapetis C, Droufakou S, et al: Avascular necrosis of bone: the hidden risk of glucocorticoids used as antiemetics in most cancers chemotherapy, International Journal of Clinical Practice 55:344�345, 2001. Vysetti S, Shinde S, Chaudhry S, et al: Phlegmasia cerulea dolens-a rare, life-threatening condition, Scientific World Journal 9:1105�1106, 2009.
Zyrtec 5 mg free shipping
Support and self-help teams play an necessary role because they allow patients to satisfy fellow sufferers allergy forecast elgin tx 10 mg zyrtec buy with visa. Conferences organized with the participation of health care practitioners have been found to be greatly appreciated (Zakrzewska et al 2009) allergy relief for dogs discount zyrtec 10 mg visa. All patients must be given enough info to allow them to become "expert" patients. Guidelines for Management No randomized controlled trials have been carried out in this group of patients. There is a single report of the therapeutic use of ketamine, and cardiac pacing has been required in sufferers with related syncope (Chong 2002). Spontaneous remission could be expected in as a lot as 75% of sufferers (Rushton et al 1981). If no evidence of neurovascular compression is discovered, full section of the glossopharyngeal nerve rootlets and higher vagal nerve rootlets should be performed, with comparable results anticipated (Resnick et al 1995, Rushton et al 1981, Kandan et al 2010). The distribution of ache involves the posterior a half of the tongue, tonsillar fossa, pharynx, and the world beneath the angle of the mandible. Clinical examination demonstrates no gross neurological deficits, however the cranial nerves must be examined rigorously to exclude the potential of a symptomatic lesion (Rushton et al 1981, Katusic et al 1991). Table 66-2 lists different concerns within the differential analysis of this disease, which incorporates tumors of the top and neck. Ferroli P, Fioravanti A, Schiariti M, et al: Microvascular decompression for glossopharyngeal neuralgia: a long-term retrospective evaluate of the Milan-Bologna experience in 31 consecutive circumstances, Acta Neurochirurgica 151:1245�1250, 2009. A prospective double-blind, randomized examine, International Journal of Radiation Oncology, Biology, Physics fifty one:449�454, 2001. Fujiwara S, Sasaki M, Wada T, et al: High-resolution diffusion tensor imaging for the detection of diffusion abnormalities within the trigeminal nerves of sufferers with trigeminal neuralgia caused by neurovascular compression, Journal of Neuroimaging 21:e102�e108, 2011. Hakanson S: Trigeminal neuralgia handled by the injection of glycerol into the trigeminal cistern, Neurosurgery 9:638�646, 1981. Headache Classification Subcommittee of the International Headache Society: the International Classification of Headache Disorders, ed 2, Cephalalgia 24:9�160, 2004. Herweh C, Kress B, Rasche D, et al: Loss of anisotropy in trigeminal neuralgia revealed by diffusion tensor imaging, Neurology sixty eight:776�778, 2007. Knafo H, Kenny B, Mathieu D: Trigeminal neuralgia: outcomes after gamma knife radiosurgery, Canadian Journal of Neurological Sciences 36:78�82, 2009. Lemos L, Flores S, Oliveira P, et al: Gabapentin supplemented with ropivacaine block of set off factors improves pain management and quality of life in trigeminal neuralgia patients when compared with gabapentin alone, Clinical Journal of Pain 24:64�75, 2008. Leonard G, Goffaux P, Mathieu D, et al: Evidence of descending inhibition deficits in atypical but not classical trigeminal neuralgia, Pain 147: 217�223, 2009. Matsushima T, Huynh-Le P, Miyazono M: Trigeminal neuralgia attributable to venous compression, Neurosurgery 55:334�337; discussion 338�339, 2004. Melzack R, Terrence C, Fromm G, et al: Trigeminal neuralgia and atypical facial pain: use of the McGill Pain Questionnaire for discrimination and analysis, Pain 27:297�302, 1986. Miller J, Acar F, Hamilton B, et al: Preoperative visualization of neurovascular anatomy in trigeminal neuralgia, Journal of Neurosurgery 108: 477�482, 2008. Mullan S, Lichtor T: Percutaneous microcompression of the trigeminal ganglion for trigeminal neuralgia, Journal of Neurosurgery fifty nine:1007�1012, 1983. A potential survey of 1052 sufferers with a view of: character of the attacks, onset, course, and character of pain, Acta Neurochirurgica 107(3�4):121�128, 1990. A potential study of 1052 sufferers with a view of: precipitating elements, related signs, objective psychiatric and neurological signs, Acta Neurochirurgica 108(3�4):100�109, 1991. A double blind managed trial, Journal of Craniomaxillofacial Surgery 18:243�246, 1990. Yomo S, Arkha Y, Donnet A, et al: Gamma Knife surgery for glossopharyngeal neuralgia, Journal of Neurosurgery a hundred and ten:559�563, 2009. Tatli M, Satici O, Kanpolat Y, et al: Various surgical modalities for trigeminal neuralgia: literature research of respective long-term outcomes, Acta Neurochirurgica a hundred and fifty:243�255, 2008. It is classed into type 1 (previously known as reflex sympathetic dystrophy) and type 2 (previously generally identified as causalgia). This view relies on scientific observations, experimentation on people, and experimentation on animals. Treatment should happen instantly and most significantly be directed towards restoration of full perform of the extremity. This goal is best attained in a complete interdisciplinary setting with particular emphasis on ache administration and restoration of operate. The key query in research is still what the mechanisms are that result in this complex syndrome. The key task to be addressed in therapy is to perform managed multicenter research that assess the acute in addition to the long-term results of drug and interventional therapies, in addition to physio- and psychotherapy. This was mainly because of the truth that diagnostic criteria were defined vaguely, underlying pathophysiological mechanisms were unknown, and therapeutic choices restricted. No information on incidence, prognosis, and prevention were obtainable; research on mechanisms targeted primarily on ache; and managed treatment research had been absent. Based on this notion it has become obvious that multiple different pathophysiological mechanisms might occur in several particular person patterns (Baron et al 2002b). Such mechanisms include somatosensory modifications (including pain) that interact with adjustments associated to the sympathetic nervous system, peripheral inflammatory changes, and adjustments within the somatomotor system (J�nig and Baron 2003). The ache is regional (not in a selected nerve territory or dermatome) and often has a distal predominance of abnormal sensory, motor, sudomotor, vasomotor edema, and/or trophic findings. In addition, sufferers reported exquisite hypersensitivity of the skin to mild mechanical stimulation. The distal finish of the extremity exhibited considerable swelling, smoothness, mottling, and in some cases, acute arthritis. He was emphatic that the sensory and trophic abnormalities spread past the innervation territory of the injured peripheral nerve and sometimes occurred distant from the location of harm. The nerve lesions giving rise to this syndrome were all the time partial; complete transection never brought on it. Because of this and the peripheral indicators of the illness, he concluded that in addition to pathology in the nerve, some course of within the pores and skin or different peripheral tissue was answerable for the pain. This notion was supported by several large clinical collection, primarily involving wounded troopers. In 1967 Richards described the scientific options of causalgia and the effect of sympatholytic interventions in tons of of instances. Precipitating occasions include fracture or minor gentle tissue trauma, low-grade an infection, frostbite or burns, and stroke and myocardial infarction. The swelling and ache usually develop at a website distant from the inciting injury, without any apparent native tissue-damaging process at the site of pain and swelling. The arm is affected extra usually than the leg, and females are affected more usually than males, with a female-to-male ratio starting from 2�4:1.
Zyrtec 10 mg buy cheap on line
The sensory pathways that convey craniofacial nociceptive enter to larger ranges of the mind originate in trigeminal ganglion nociceptors and their related nuclei throughout the trigeminal mind stem sensory complicated and higher cervical spinal cord allergy shots effects on immune system purchase zyrtec 5 mg. In all mammals, the ophthalmic branch provides the cornea, neighboring conjunctiva, skin of the dorsum and tip of the nostril, intranasal mucosa, dorsum of the pinnacle, upper eyelid, and supraorbital pores and skin allergy testing qld health 5 mg zyrtec buy otc. Some components of the pinnacle obtain their sensory innervation from branches of the upper cervical nerves (C2 and C3). Each division provides one of the three totally different dermatomes of the face and the underlying deeper mucosal, vascular, muscular, and meningeal tissues. The maxillary division contains the infraorbital and postorbital skin, upper lip, lateral facet of the nose, intraoral maxillary mucosa, and upper tooth. The mandibular department supplies the temporomandibular joint, lower lip pores and skin, intraoral mandibular mucosa, decrease tooth, and anterior part of the tongue. Transmission of acute pain involves the activation of different teams of sensory receptors on peripheral A and C fibers, the nociceptors, which reply to noxious mechanical, thermal, and chemical stimuli. The roles of those receptors in nociceptive signaling are covered in Chapters 1 to four. An approximate somatotopic organization exists within the trigeminal ganglion of mammals, with ophthalmic cells mendacity anteromedially, mandibular cells mendacity posterolaterally, and maxillary cells in between. Central processes of those major afferents enter the mind stem via the trigeminal tract in a dorsal and lateral position, adjacent to the trigeminal motor root. After coming into the tract, most afferents pass caudally while giving off collaterals that terminate in the subdivisions of the spinal trigeminal nucleus and upper cervical wire to activate second-order neurons. After getting into the trigeminal tract, most afferents cross caudally whereas giving off collaterals that terminate within the subdivisions of the spinal trigeminal nucleus and higher cervical cord to activate second-order neurons. The spinal trigeminal sensory nucleus (Sp5) consists of three subnuclei (oralis, Sp5O; interpolaris, Sp5I; and caudalis, Sp5C). A and C primary afferents fibers terminate somatotopically in a dorsal�ventral style, with mandibular afferents ending dorsally (V3), maxillary fibers projecting centrally (V2), and ophthalmic fibers innervating the ventral-most aspect of Sp5 (V1). C1, first cervical phase of the spinal cord; Cu, cuneate nucleus; Pr5, principal sensory trigeminal nucleus. A and C primary afferent fibers terminate somatotopically in a dorsal�ventral trend, with mandibular afferents ending dorsally, maxillary fibers projecting centrally, and ophthalmic fibers innervating the ventral-most facet of Sp5. In Sp5C this sample changes and turns into a segmental "onion skin" association, with enter from the nostril and rostral a half of the face ending rostrally and the posterior craniofacial areas terminating steadily at more caudal ranges. Sp5C is the only portion that has a laminated structure and a morphological and functional group corresponding to the spinal dorsal horn. In contrast to hair afferents, which have extra compact, circumscribed arbors, these of nociceptors from the pores and skin, cranial blood vessels, dura, mucosa, temporomandibular joint, or tooth pulp have a widespread termination. Small-diameter fibers lengthen throughout the trigeminal tract and then terminate primarily within the Sp5I�Sp5C junction and Sp5C, where they typically present collaterals that contact the dendrites and somata of many hundreds of trigeminal neurons. In addition to this widespread distribution of nociceptive enter, the phenomenon of convergence onto a single central neuron receiving input from different primary afferents is a characteristic that distinguishes the trigeminal advanced and has been proposed to clarify referral of ache and the problem sometimes encountered in precise localization of a painful focus. Moreover, toothache typically radiates to the neighboring facial and neck regions, whereas muscle, cervical, auricular, and even cardiac ache could project to the orofacial areas. As acknowledged beneath, this phenomenon of pain referral is amplified following peripheral and subsequent central sensitization. They thus present convergence of exteroceptive (cutaneous) and interoceptive (meningeal, muscle, dental pulp) enter (Sessle et al 1986, Burstein et al 1998, Shimizu et al 2009). They additionally reply to a big selection of other stimuli (innocuous thermal and/or noxious and chemical stimuli) and exhibit cutaneous and deep tissue convergence (Sessle 2000). Sp5C sensitized neurons have decrease thresholds to each dural and peri-ocular skin stimulation and show a significant enhance within the dimension of their dural and cutaneous receptive fields. Based on these findings, it was proposed that the referred, cutaneous allodynia noticed in migraine sufferers is as a result of of central sensitization of Sp5C neurons following peripheral sensitization of meningeal nociceptors (Burstein et al 1998). Moreover, the ophthalmic region of Sp5C, which accommodates neurons that obtain convergent enter from the dura and peri-orbital skin, sends projections to the ophthalmic main afferent projection area of the contralateral trigeminal brain stem sensory complicated. These projections are somatotopically organized and extend rostrocaudally from the caudal spinal trigeminal nucleus to the upper cervical dorsal horn C2�3 segments (Jacquin et al 1990b, Noseda et al 2008). In the final century, neurosurgical procedures have shown that transection of the trigeminal descending tract at the degree of the rostral pole of Sp5C produces thermal analgesia of the face with out significantly affecting tactile sensations (Sj�qvist 1939). However, painful sensations from the oral cavity have been partially preserved following tractotomy, thus suggesting that craniofacial noxious enter can be conveyed by neurons located more rostrally. Animal studies have confirmed that orofacial tissues 796 Section Six Clinical States/Headache and Facial Pain and in flip activate lamina I neurons (Miraucourt et al 2007, Basbaum et al 2009, Nakajima et al 2011). Such input might turn into efficient following long-lasting noxious stimulation of meningeal nociceptors and thus contribute to the central sensitization that occurs after long-lasting migraine assaults (Burstein et al 2000a). In patients it might elicit the cutaneous allodynia that extends outdoors the referred pain space to the pores and skin over the contralateral head and forearm (Burstein et al 2000b). Sp5C also projects to the ipsilateral junction of Sp5C and Sp5I, Sp5O, and Pr5 nuclei over their complete caudal�rostral extent (Bereiter et al 2000, Woda et al 2001). Such intratrigeminal connections are somatotopically organized, as observed in both animals (Jacquin et al 1990a) and people (DaSilva et al 2002); nevertheless, the functional significance of those topographically organized, intratrigeminal connections has not been fully elucidated. Ipsilateral input from Sp5C neurons to rostral trigeminal nuclei could contribute to the amplification of nociceptive output to supramedullary buildings through the interpolar, oral, and principal subdivisions since these regions convey orofacial input to the brain stem and thalamic areas (Peschanski 1984, Jacquin et al 1989). As in spinal nociceptive processing, glutamatergic transmission is essential in Sp5C since native software of glutamate activates nociceptive neurons (Henry et al 1980). There is also sturdy proof that rostral trigeminal nuclei, especially Sp5O, convey each extra- and intra-oral nociceptive enter, which depends on glutamatergic input from Sp5C (Parada et al 1997, Woda et al 2001). Recent studies have shown that following intense noxious stimulation or nerve injury, nice primary afferents launch glutamate and several other other peptides and neuromodulators onto lamina I neurons. Under such circumstances, lamina I nociceptive neurons may be activated by A non-nociceptive primary afferents that normally drive inhibitory interneurons. It also tasks to the hypothalamic ventromedial nucleus, which participates in meals intake (Bernard et al 1995). Schematic illustration of the principle ascending projections from superficial (left) and deep (right) medullary trigeminal neurons. Lamina I trigeminal medullary neurons send nociceptive and thermal signals to the spinal, bulbar, and telencephalic regions implicated in autonomic, emotional, and somatosensory processing. Rather than subserving only ache processing, these circuits could contribute to sustaining primary emotional and motivational states. Deep trigeminal medullary neurons are able to convey a variety of indicators originating both from the external environment by way of the pores and skin or from the internal organs. They send enter to a quantity of regions implicated in somatosensory, motor, arousal, and attentional processing of nociceptive input. In truth, this could be a functionally heterogeneous space constituted by adjoining zones implicated in attentional, motor, and autonomic reactions that might permit it to elicit varied behavioral reactions (Vogt 2005). This suggests that the ventral posterior areas could subserve spatial discrimination. Furthermore, single-unit recordings from a caudal ventral region of the thalamus in humans have proven neurons that could probably be activated by noxious stimuli and that stimulation of this region induces thermal and/or painful sensations (Lenz and Dougherty 1997). The ventral, medial, and posterior aspects of the rat thalamus are innervated by trigeminal lamina I neurons (around 15% of the entire population of lamina I projecting neurons).
Best zyrtec 5 mg
In youngsters, 25% of these referred for analysis of chest ache had abnormal esophageal motility (Glassman et al 1992) allergy shots needle size zyrtec 10 mg discount otc. Psychological elements can affect esophageal motility (Rubin et al 1962) and will influence the signs and symptoms of esophageal motility issues allergy shots chicago zyrtec 5 mg on line. An important supply of esophageal dysmotility related to ache therapy is opioid use (Kraichely et al 2010). Esophageal perforation can be traumatic, iatrogenic, or "spontaneous" or be attributable to the ingestion of chemicals or foreign bodies (Younes and Johnson 1999, Wu et al 2007). Violent esophageal exercise also can lead to Mallory-Weiss tears on the gastroesophageal junction and esophageal hematomas. The ache accompanying esophageal perforation and esophageal hematoma may be interpreted as myocardial ischemia, pulmonary embolisms, and aortic dissection (Smith et al 1974, Curci and Horman 1976, Symbas et al 1978). Fever with mediastinal and subcutaneous emphysema usually accompanies esophageal perforation. In addition to pain of esophageal origin, a spectrum of life-threatening and extra benign stomach processes (see Table 52-3) can also be manifested as thoracic pain, often by way of stimulation of the diaphragm and, therefore, with radiation to the shoulder. Musculoskeletal System, Chest Wall, and Breast Disorders of the musculoskeletal system, breast, and chest wall (see Box 52-1) are regularly the supply of thoracic pain in grownup (see Table 52-1) and pediatric populations (see Table 52-2) and, not infrequently, masquerade as myocardial ischemia (Epstein et al 1979, Fam and Smythe 1985, Christensen et al 2005). Chest wall syndromes were current in 28% of patients admitted to the hospital for acute chest pain and were the only prognosis in 12% (Fruergaard et al 1996). Many of those situations are benign, others probably disabling, and some the manifestation of systemic illness. The ribs, their articulations, the clavicle, the sternum, and the spine are the origin of a substantial variety of painful situations. Pain from rib fractures, minor trauma, and coughing may be the supply of extreme pleuritic ache. The slipping rib syndrome is considered traumatic in origin and is characterized by elevated mobility of one of many lower ribs, generally the 10th, which leads to severe sharp ache on the anterior costal margin (Mynors 1973). Traumatic anterior or posterior dislocation and systemic and metastatic illness can lead to pain originating from the sternoclavicular joint (Fam and Smythe 1985). Systemic illness also can involve the manubriosternal joint (Fam and Smythe 1985). The spectrum of rheumatological syndromes that can lead to chest pain originating from the bones and 728 Section Five Clinical States/Viscera 1953). The pain could additionally be intensified by respiratory activity, though occasionally pleural involvement is present. Fibromyalgia (see Chapter 48) is characterised by persistent musculoskeletal ache, tender points, and sleep disturbances and can result in pain of thoracic origin. Fibromyalgia is commonly the cause for chest pain not of cardiac origin, with estimates starting from 3�30% of non-cardiac chest ache (Almansa et al 2010); the disparity among research in all probability displays the patient inhabitants and diagnostic standards for fibromyalgia. Those undergoing catheterization, even with normal coronary arteries, had been extra prone to describe symptoms of melancholy. As already indicated, ache of spinal origin may be the most typical reason for thoracic pain in these seen in specialised pain clinics (Bonica and Sola 1990, van Kleef et al 1995). Disc herniation is less frequent within the thoracic backbone than within the cervical and lumbar spine, generally entails the decrease thoracic segments, and may produce radicular pain suggestive of myocardial ischemia (Hamberg and Lindahl 1981, McInerney and Ball 2000). A host of other native and systemic conditions can lead to thoracic pain of spinal origin, although these circumstances are generally associated with pain in the posterior chest wall. Arthritis of the costovertebral and costotransverse joints can end result in thoracic backache that can worsen with respiratory effort (Nathan et al 1964). The mobility of the 1st, 11th, and twelfth ribs results in the next prevalence of degenerative changes in these joints, and arthritis of the first costovertebral joint may cause thoracic outlet syndrome (Weinberg et al 1972). Ankylosing spondylitis can produce ache within the backbone and its articulation with the ribs and will limit chest tour. This pain can typically radiate to the anterior aspect of the chest and be a consideration in the differential prognosis of myocardial ischemia (Good 1963). Articulations of the sternum, clavicle, ribs, and xiphoid may be simultaneously affected. Finally, when current within the cervical spine, most of the identical pathological processes of the thoracic spine produce chest pain because afferent nerve fibers from the heart synapse in the decrease cervical backbone. The term cervicothoracic angina displays the ability of pathology of the cervical and thoracic backbone to supply ache that mimics that of myocardial ischemia (Christensen et al 2005). Although infectious and malignant processes can lead to thoracic pain originating in the breast, extra benign causes are sometimes the reason for breast ache. Breast pain enough to cause misery and intervene with every day activities occurred in 68% of girls self-referred to a breast screening clinic over the course of a year (Leinster et al 1987). Cyclic mastodynia waxes and wanes with the menstrual cycle and accounts for approximately 67% of instances. It typically occurs in the third decade of life and causes a boring burning or aching pain in both breasts. Compression of any of the neurovascular structures passing by way of the thoracic outlet can lead to thoracic outlet syndrome, with the signs and symptoms relying on whether or not neural, venous, or arterial parts are concerned (Peet et al 1956, Pin et al 2010). Neurogenic thoracic outlet syndrome is as a result of of physiological compression of the brachial plexus as it passes via the interscalene triangle (Brantigan and Roos 2004a), and it accounts for 95% of cases of thoracic outlet syndrome. Muscle fibrosis and scar tissue in the anterior scalene muscle attributed to persistent irritation are outstanding pathological features (Machleder et al 1986). A history of trauma involving the higher extremity or extremes of repetitive movement is commonly elicited. Symptoms embody paresthesias and weakness of the higher extremity and varying levels of pain within the head, neck, shoulder, and axilla with radiation down the arm, and it has a considerable influence on high quality of life (Chang et al 2009). The prognosis of neurogenic thoracic outlet syndrome is commonly difficult to make, with the signs initially being attributed to a selection of different situations (Brantigan and Roos 2004b). Venous thoracic outlet syndrome accounts for 5% of cases of thoracic outlet syndrome and could be acute or continual. Symptoms come up from positional venous obstruction or effort-related thrombosis of the axillosubclavian vein and might embody cyanosis, swelling, and ache in the arm, usually with a historical past of previous vigorous activity (Illig and Doyle 2010). Chronic venous thoracic outlet syndrome is regularly iatrogenic and associated to using venous entry catheters. Though accounting for lower than 1% of instances of thoracic outlet syndrome, arterial thoracic outlet syndrome can threaten limb survival. Although the symptoms are sometimes these of limb ischemia from subclavian artery thromboembolism, signs of arterial thoracic outlet syndrome can also overlap those of neurogenic thoracic outlet syndrome (Criado et al 2010). Neurovascular compression by the pectoralis minor, often recognized as pectoralis minor syndrome, can result in signs similar to these of thoracic outlet syndrome, can co-exist with thoracic outlet syndrome, or could additionally be diagnosed unbiased of thoracic outlet syndrome (Sanders and Rao 2010). Thoracic ache of myofascial origin is common, is typically mistaken for the pain of myocardial ischemia, and infrequently co-exists with anginal ache (Epstein et al 1979, Christensen et al 2005). Pain and tenderness within the intercostal, pectoral, and other muscle tissue of the thorax are frequent following vigorous exercise or coughing. Tenderness over the chest wall in affiliation with different symptoms can also be seen with pectoralis minor syndrome (Sanders and Rao 2010).
Discount zyrtec 5 mg fast delivery
Post�Radical Neck Dissection Pain Chronic neck and shoulder ache after radical neck dissection is common (Dijkstra et al 2001) allergy gif purchase zyrtec 5 mg mastercard. In other instances it can outcome from musculoskeletal imbalance within the shoulder girdle following Aromatase Inhibitor Pain Syndromes Aromatase inhibitor remedy for the therapy of hormoneresponsive breast cancer is commonly accompanied by musculoskeletal pain and stiffness allergy symptoms heart racing order zyrtec 10 mg fast delivery. Common manifestations embody hand osteoarthritis, tendonitis, set off finger, and carpal tunnel syndrome. Pain was extreme in 30%, continuous in 41%, central in 50%, and peripheral in 79% and resulted in discontinuation of the drug in 20% of patients (Presant et al 2007). Chronic Pain Associated with Bisphosphonate Therapy Osteonecrosis of the Jaw Osteonecrosis of the jaw is described as an intraoral complication after the intravenous administration of nitrogen-containing bisphosphonates. It is an unusual complication whose incidence rate has climbed in current years (Migliorati et al 2010). It is outlined as an sudden improvement of necrotic bone in the oral cavity and is commonly related to administration of the bisphosphonates pamidronate and zoledronate. Symptoms can mimic routine dental issues corresponding to decay or periodontal illness (Migliorati et al 2006). Osteonecrosis of the jaw is also usually correlated with earlier dental procedures throughout bisphosphonate remedy, similar to tooth extractions. To reduce this danger, clinical dental examination and a panoramic jaw radiograph ought to be performed before sufferers start bisphosphonate remedy; dental treatment and different oral procedures ought to be accomplished earlier than initiating bisphosphonate therapy, and sufferers must be informed and instructed in regards to the significance of sustaining good oral hygiene and having regular dental evaluation (Cavanna et al 2007). Chronic Diffuse Pain In June 2008 the Food and Drug Administration issued a special warning regarding the potential of severe and typically incapacitating bone, joint, and/or muscle (musculoskeletal) pain in patients taking bisphosphonates. The severe musculoskeletal ache could occur within days, months, or years after beginning bisphosphonate treatment. Some sufferers have reported complete reduction of signs after discontinuing the bisphosphonate, whereas others have reported sluggish or incomplete decision. The threat factors for and incidence of extreme musculoskeletal pain related to bisphosphonates are unknown (Lenzer 2008). Chronic Post-surgical Pain Syndromes Surgical incision at just about any location may result in continual pain. In contrast, a number of syndromes are now clearly acknowledged as sequelae of specific surgical procedures. The predominant underlying pain mechanism in these syndromes is neuropathic because of injury to peripheral nerves or plexus. Breast Surgery Pain Syndromes Chronic pain of variable severity is a standard sequela of surgical procedure for breast most cancers. Similar to droopy shoulder syndrome (Swift and Nichols 1984), this syndrome may be complicated by the event of thoracic outlet syndrome or suprascapular nerve entrapment, with selective weak spot and losing of the supraspinatus and infraspinatus muscular tissues (Brown et al 1988). These lesions could additionally be difficult to diagnose in tissues broken by radiation and surgery. Empirical therapy with antibiotics should be thought-about (Bruera and MacDonald 1986, Coyle and Portenoy 1991). Post-Thoracotomy Pain Two major research of post-thoracotomy ache have been performed (Kanner et al 1982, Keller et al 1994). In the first (Kanner et al 1982), three teams have been recognized; the largest (63%) had prolonged postoperative ache that abated within 2 months after surgical procedure. Recurrent ache following decision of the postoperative pain was normally because of neoplasm. A second group (16%) experienced pain that endured following thoracotomy after which increased in depth during the followup period. Local recurrence of disease and infection have been the commonest causes of the rising ache. A ultimate group had a chronic period of secure or decreasing pain that steadily resolved over a most 8-month interval. Overall, the development of late or growing post-thoracotomy pain was due to recurrent or persistent tumor in more than 95% of patients. This finding was corroborated in the more modern research, which evaluated the data of 238 consecutive sufferers who underwent thoracotomy; recurrent ache was identified in 20 patients, all of whom were discovered to have tumor regrowth (Keller et al 1994). In some sufferers, post-thoracotomy ache seems to be attributable to a taut muscular band inside the scapular area. In such cases the ache may be amenable to trigger level injection of local anesthetic (Hamada et al 2000). Postoperative Frozen Shoulder Patients with post-thoracotomy or post-mastectomy ache are at risk for the development of frozen shoulder (Maunsell et al 1993). This lesion might become an unbiased focus of pain, significantly if difficult by reflex sympathetic dystrophy. Adequate postoperative analgesia and lively mobilization of the joint soon after surgical procedure are essential to stop these problems. Phantom Pain Syndromes Phantom limb pain is perceived to arise from an amputated limb, as if the limb were nonetheless contiguous with the body. Phantom pain is skilled by 60�80% of sufferers following limb amputation but is severe in solely about 5�10% of instances (Ehde et al 2000, Nikolajsen and Jensen 2000, Flor 2002). The incidence of phantom pain is significantly higher in patients with a long period of pre-amputation ache and in those with pain on the day earlier than amputation (Weinstein 1994, Nikolajsen et al 1997b). Patients who had pain earlier than 1059 the amputation could expertise phantom pain that replicates the sooner one (Katz and Melzack 1990). Phantom ache is extra prevalent after tumor-related than after traumatic amputations, and postoperative chemotherapy is an additional risk factor (Smith and Thompson 1995, Flor 2002). The pain may be steady or paroxysmal and is frequently associated with bothersome paresthesias. The phantom limb might assume painful and weird postures and will gradually telescope and strategy the stump. There is growing proof that preoperative or postoperative neural blockade reduces the incidence of phantom limb ache in the course of the first yr after amputation (Pavy and Doyle 1996, Enneking and Morey 1997, Katz 1997, Nikolajsen et al 1997a). Recurrence of ache after such a remission or late onset of pain in a beforehand painless phantom limb suggests the looks of a more proximal lesion, together with recurrent neoplasm (Chang et al 1997). Phantom breast ache after mastectomy, which occurs in 15�30% of patients (Kroner et al 1989, Kwekkeboom 1996, Tasmuth et al 1996, Rothemund et al 2004, Dijkstra et al 2007), additionally seems to be related to the presence of preoperative pain (Kroner et al 1989). The pain tends to begin in the region of the nipple and then spreads to the entire breast. The character of the pain is variable and may be lancinating, continuous, or intermittent (Kroner et al 1989, Rothemund et al 2004). A phantom rectum pain syndrome occurs in approximately 15% of sufferers who bear abdominoperineal resection of the rectum (Ovesen et al 1991, Boas et al 1993). Phantom rectal ache could develop either in the early postoperative period or after a latency of months to years. Late-onset ache is nearly at all times related to tumor recurrence (Ovesen et al 1991, Boas et al 1993). Rare cases of phantom bladder pain after cystectomy and phantom eye ache after enucleation have additionally been reported. Stump Pain Stump ache occurs at the website of the surgical scar a number of months to years following amputation (Davis 1993). This pain is characterized by burning or lancinating dysesthesias, which are often exacerbated by motion or stress and blocked by injection of an area anesthetic.